
Epidemiology
The geographic range of Coccidioides has been derived from clinical cases, soil testing, and on the basis of skin testing performed in 1957 throughout the Southwestern United States (1, 2). The exact ecologic niche remains to be determined. Endemic areas where disease is prevalent include Arizona, California, New Mexico, Nevada, Utah, Washington, Texas, Mexico, and some areas in Guatemala, Honduras, Venezuela, Brazil, Argentina, and Paraguay (3, 4). In the United States, the annual incidence of coccidioidomycosis is variable, but overall is rising, from a rate of 5.3 per 100,000 in 1998 to a rate of 42.6 in 2011 (5). Of these cases reported to the Centers for Disease Control, 66% were from Arizona and 31% from California. Despite the increased incidence, from an analysis of death certificates, the age-adjusted mortality rate from 1990 - 2008 has remained stable at ~0.59 per million person years (6). There were 1,451 coccidioidomycosis-related deaths in California compared to 1,010 in Arizona despite its higher annual reported case rate.
Number of coccidioidomycosis cases and incidence rate, by estimated year of illness onset* — California, 1995–2016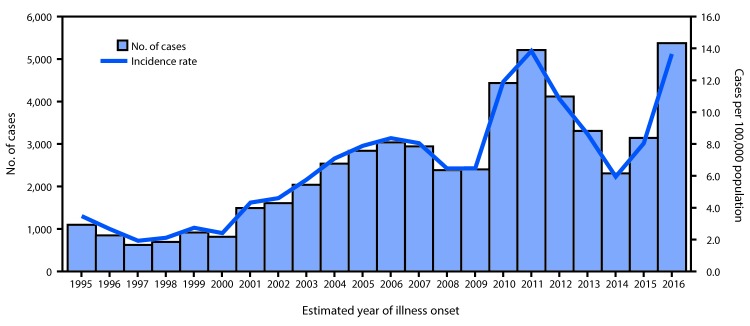
MMWR Morb Mortal Wkly Rep. 2017 Aug 11; 66(31): 833–834
The incidence of coccidioidomycosis in California and Arizona can vary greatly by geographic region, and may be seasonal in pattern. In a yearly summary by the California Department of Health, the overall incidence of coccidioidal infection in the state rose from 4.3 to 11.6 per 100,000 population between 2001 and 2010 (7). In Kern County, however, the rate reported in 2011 was much higher, 241 per 100,000 population (8). Similar increases have been observed in Arizona (9, 10). The reasons for the overall increase are not fully clear, and have been attributed to changing environmental conditions, human activities in endemic areas, changing surveillance methods and definitions, increased numbers of immunosuppressed individuals, and even improved awareness and diagnostic testing rates(11). In endemic regions, the people most affected are construction and farm workers, military personnel, archaeologists, excavators, inmates, and officers in correctional facilities.
Epidemics in endemic regions have occurred after dust storms, earthquakes, and earth excavation where dispersion of arthroconidia is facilitated (9, 12). In Washington State, three cases were recently reported, an area not previously considered endemic; follow-up soil testing showed the presence of Coccidioides immitis, suggesting the geographic range of this organism is larger than previously thought (13, 14). After coccidioidomycosis became a reportable condition, the case rate even in nonendemic regions (eg recent report in Missouri) increased substantially, but many cases were among people who never previously travelled to an endemic region and were diagnosed serologically rather than by culture, PCR or histopathologically (15). Clinical cases of coccidioidomycosis in patients from non-endemic regions are often reported, but frequently a link is established, however brief the transit, to an endemic region (16). There is even a case report of coccidioidomycosis in Hong Kong in a patient who is believed to have contracted the disease by sweeping shipping containers from the US with no other link to the endemic region (17).
REFERENCES
- Brown J, Benedict K, Park BJ, Thompson GR, 3rd. Coccidioidomycosis: epidemiology. Clinical epidemiology 2013; 5: 185-97.
- Edwards PQ, Palmer CE. Prevalence of sensitivity to coccidioidin, with special reference to specific and nonspecific reactions to coccidioidin and to histoplasmin. Diseases of the chest 1957; 31(1): 35-60.
- Talamantes J, Behseta S, Zender CS. Statistical modeling of valley fever data in Kern County, California. International journal of biometeorology 2007; 51(4): 307-13.
- Stevens DA. Coccidioidomycosis. The New England journal of medicine 1995; 332(16): 1077-82.
- Centers for Disease C, Prevention. Increase in reported coccidioidomycosis--United States, 1998-2011. MMWR Morbidity and mortality weekly report 2013; 62(12): 217-21.
- Huang JY, Bristow B, Shafir S, Sorvillo F. Coccidioidomycosis-associated Deaths, United States, 1990-2008. Emerging infectious diseases 2012; 18(11): 1723-8.
- Curfs-Breuker IM D-OY, Endtz HP, Verweij PE, Meis JF. . In Vitro Activity of Caspofungin compared with Six other Antifungal Agents against 239 Prospectively Collected Clinical Aspergillus Isolates from the Netherlands. In: Programs and Abstracts of the 3rd Advances Against Aspergillosis Annual Meeting. Miami: 2008. Poster 37.
- Curfs-Breuker IM MJ, Debets-Ossenkopp YJ, Endtz HP, Verweij PE, Meis JF. . In Vitro Activity of Isavuconazole (BAL4815) Compared with Seven other Antifungal Agents against 309 Prospectively Collected Clinical Candida Isolates from the Netherlands. In: Programs and Abstracts of the 17th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID). Munich: 2007. Poster P1978.
- Ampel NM. Coccidioidomycosis: a review of recent advances. Clinics in chest medicine 2009; 30(2): 241-51, v.
- Parish JM, Blair JE. Coccidioidomycosis. Mayo Clinic proceedings 2008; 83(3): 343-48; quiz 8-9.
- Thompson GR, 3rd. Pulmonary coccidioidomycosis. Seminars in respiratory and critical care medicine 2011; 32(6): 754-63.
- Schneider E, Hajjeh RA, Spiegel RA, et al. A coccidioidomycosis outbreak following the Northridge, Calif, earthquake. JAMA : the journal of the American Medical Association 1997; 277(11): 904-8.
- Litvintseva AP, Marsden-Haug N, Hurst S, et al. Valley fever: finding new places for an old disease: Coccidioides immitis found in Washington State soil associated with recent human infection. Clin Infect Dis 2015; 60(1): e1-3.
- Marsden-Haug N, Goldoft M, Ralston C, et al. Coccidioidomycosis acquired in Washington State. Clin Infect Dis 2013; 56(6): 847-50.
- Turabelidze G, Aggu-Sher RK, Jahanpour E, Hinkle CJ. Coccidioidomycosis in a State Where It Is Not Known To Be Endemic - Missouri, 2004-2013. MMWR Morbidity and mortality weekly report 2015; 64(23): 636-9.
- Baddley JW, Winthrop KL, Patkar NM, et al. Geographic distribution of endemic fungal infections among older persons, United States. Emerging infectious diseases 2011; 17(9): 1664-9.
- Tang TH, Tsang OT. Images in clinical medicine. Fungal infection from sweeping in the wrong place. The New England journal of medicine 2011; 364(2): e3.

 Karryn Doyle, CCEP
Karryn Doyle, CCEP