
Residency Program - Case of the Month
January 2011 - Presented by Mahan Matin, M.D.
Clinical history:
The patient is a 22-year-old woman with a 10 year history of menorrhagia. At age 18, she underwent dilation & curettage for presumed incomplete abortion after presenting with increased vaginal bleeding and elevated quantitive beta-hCG. The tissue obtained was diagnosed as endometrial polyp, rather than products of conception. She continued to have vaginal bleeding and elevated beta-hCG levels, undergoing multiple hysteroscopy exams with D&C for recurrent masses found protruding from the cervix, with tissue specimens over time diagnosed as benign polyps, adenomyoma, and "infarcted endometrial polyp." Due to persistent vaginal bleeding uncontrolled by medications, and an enlarged uterus in the setting of elevated beta-hCG levels ranging up to 90.9, there was concern for gestational trophoblastic disease. A hysterectomy was performed.
Gross description:
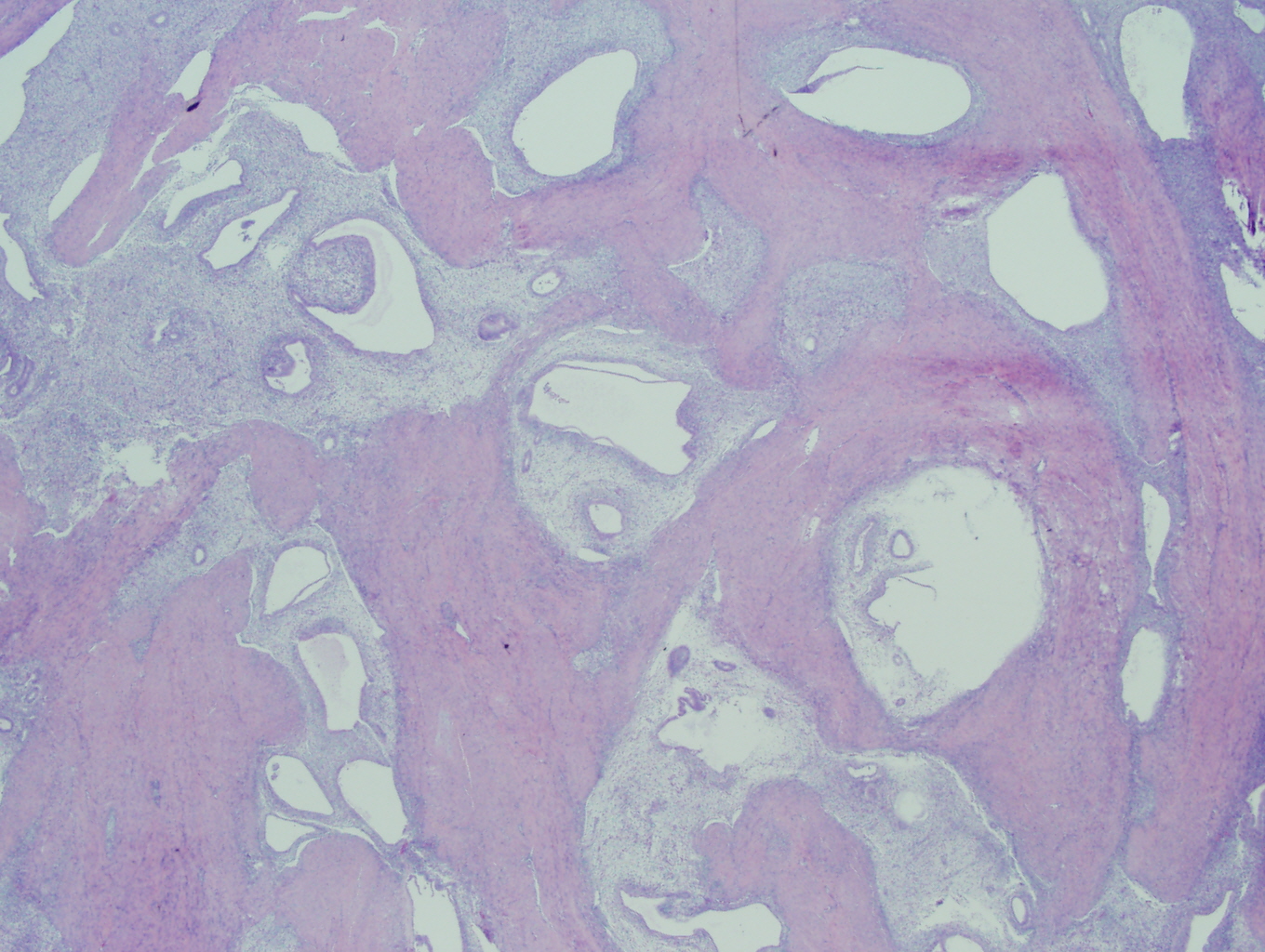
Received fresh was a previously opened 17x12x9 cm (1292 g) uterus and cervix with a purple-brown polypoid mass on the anterolateral serosa. There were two tan polypoid masses (8x5 cm and 5x3 cm) with hemorrhagic areas within the endometrial cavity that invaded 2 cm into the 4 cm thick myometrium.
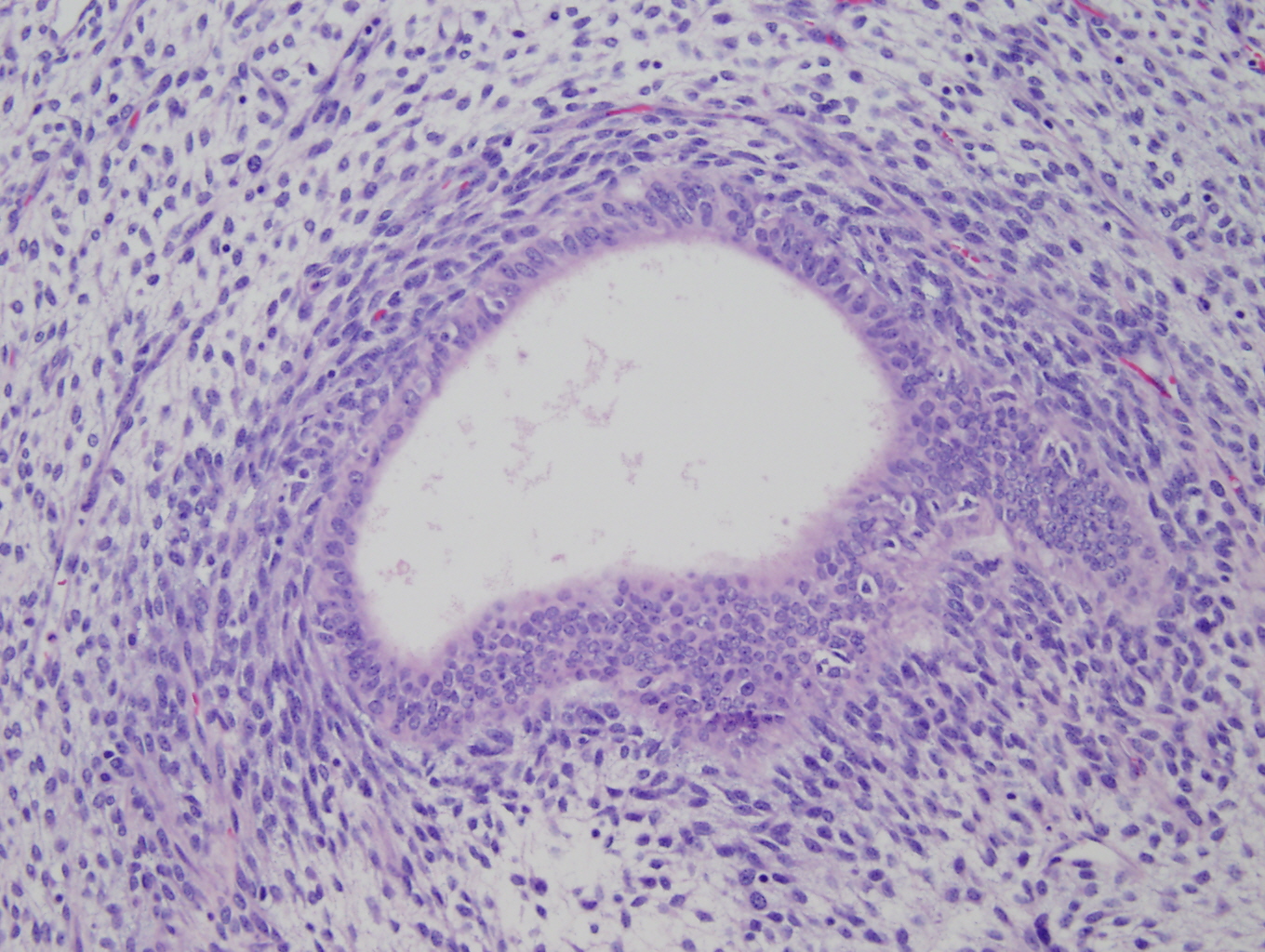
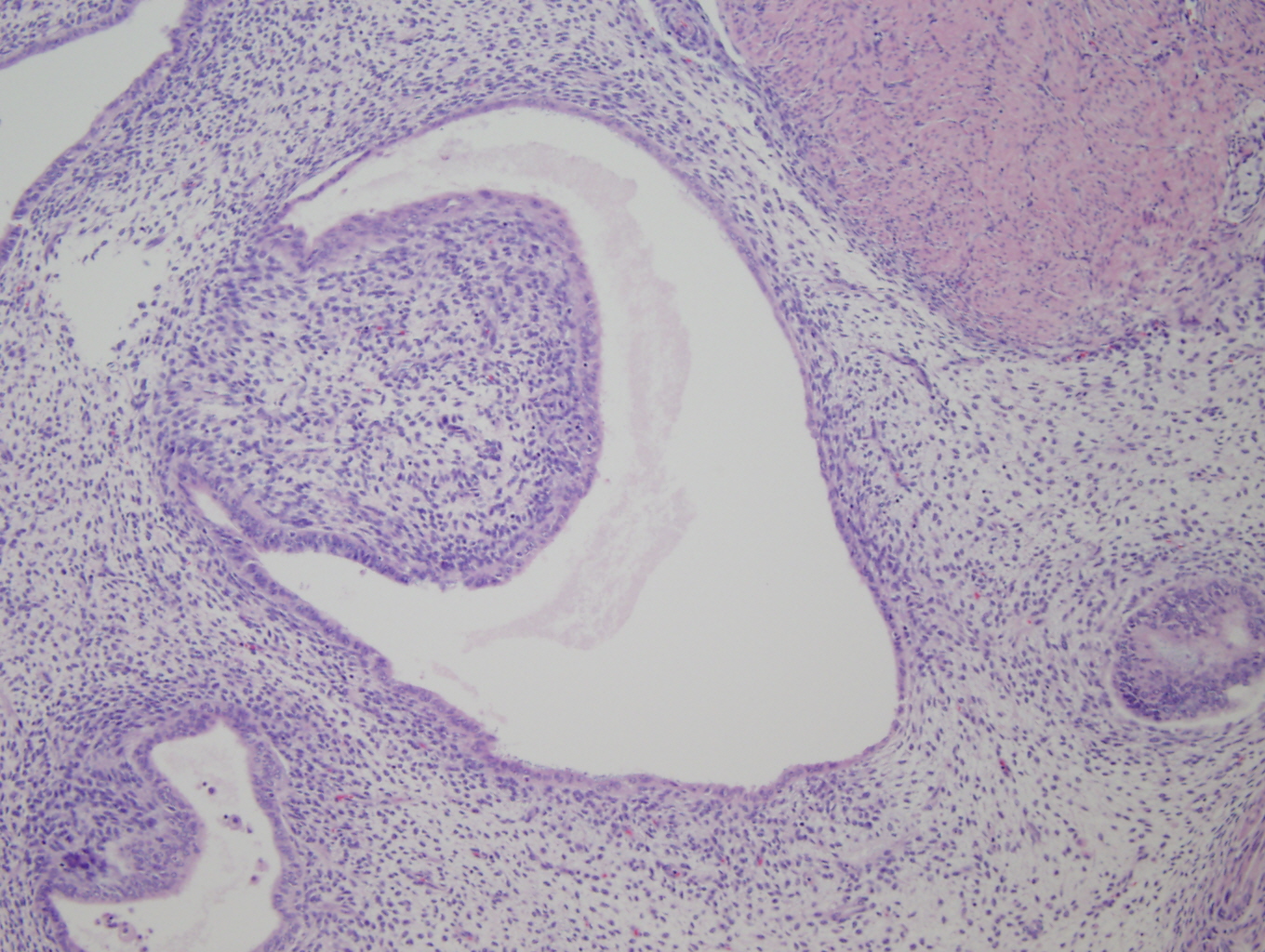
Microscopic Photographs:
 |
 |
 |
 |
 Meet our Residency Program Director
Meet our Residency Program Director