
Resident Program - Case of the Month
March 2019 - Presented by Peter Conner (Mentored by Mirna Lechpammer)
Clinical History
A 43-year-old female presented to the emergency department with a seizure. She has history of alcoholism and seizures attributed to alcohol withdrawal. She reported that she had been binge drinking for the past two days.
Radiologic Findings
An MRI of the head was performed which revealed a focal mass lesion in the right parietotemporal junction. Hemorrhage was seen within the middle of the mass and had non-homogeneous enhancement. (See Figures 1 and 2).
Click on image to enlarge.
Figure 1 - T1 MRI sagittal plane cross-section of the mass at the parietotemporal junction.
Figure 2 - T2 MRI transverse plane cross-section of the mass at the parietotemporal junction.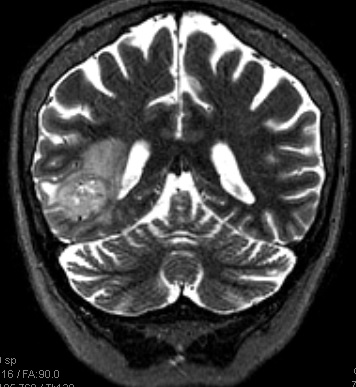
Pathological Findings
Microscopic examination of the brain mass reveals the tumor is composed of atypical astrocytes with frequent mitoses, vascular proliferation and pseudopalisading necrosis. Additional immunohistochemistry was performed which showed the following:
SOX2: Positive
SOX10: Negative
GFAP: Positive
OLIG2: Positive in approximately 70% of tumor cells
ATRX: Retained in more than 90% of tumor cells
P53: Positive in approximately 10% of tumor cells
The MIB-1 proliferative index is approximately 30%
IDH1 (R132H) IHC is negative.
(See figures 3-7 for images of selected slides)
Click on image to enlarge.
Figure 3 - H&E from frozen section analysis. (40X Magnification)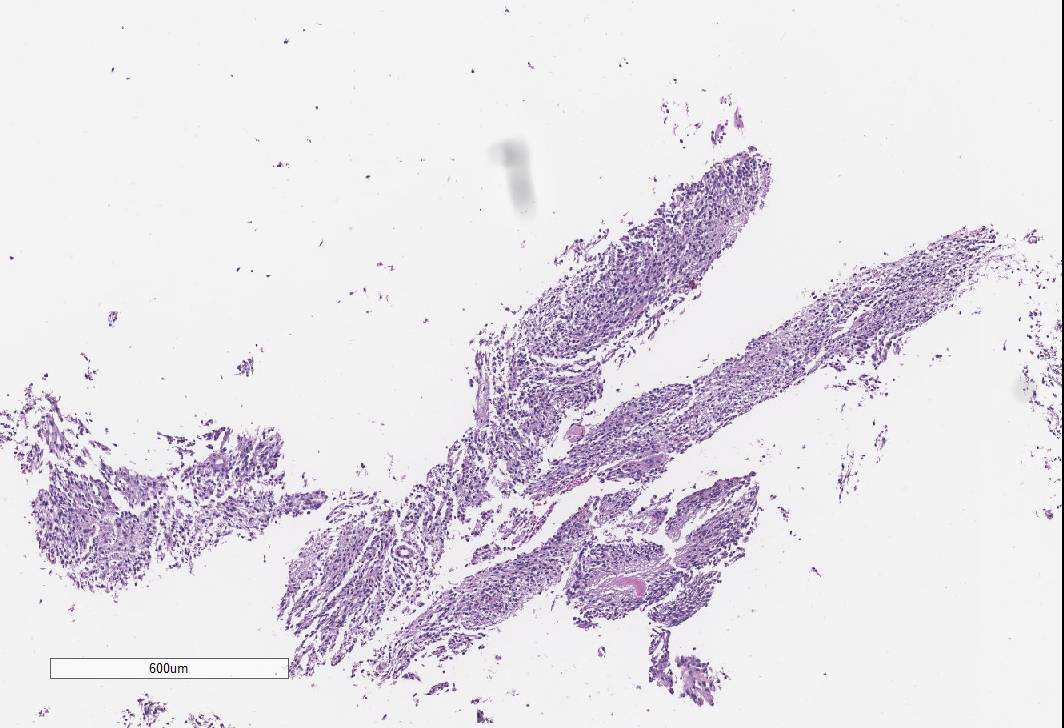
Figure 4 - H&E from embedded specimen. (100X Magnification)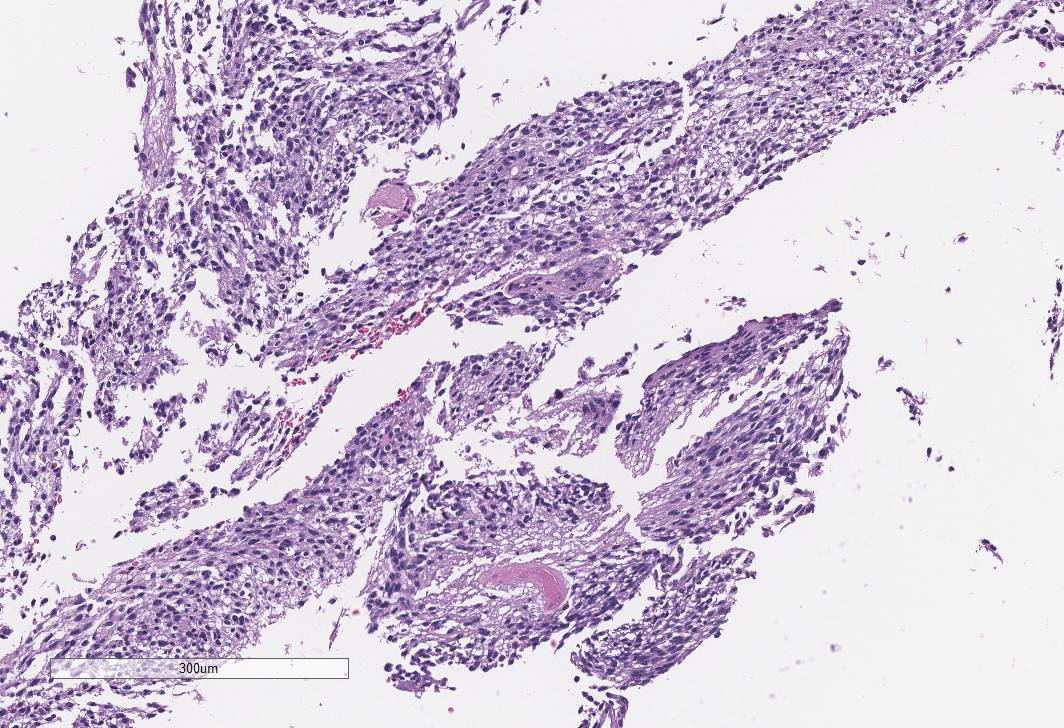
Figure 5 - ATRX stained immunohistochemistry showing positivity in 90% of tumor cells (40X magnification)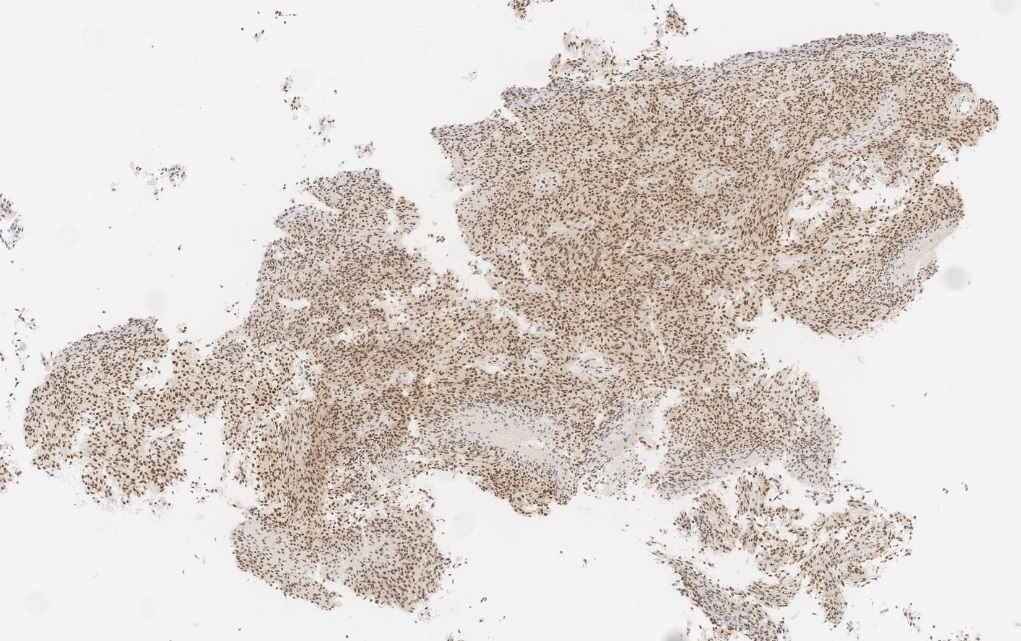
Figure 6 - Ki-67 immunohistochemistry showing a proliferative index of approximately 30%. (40X Magnification)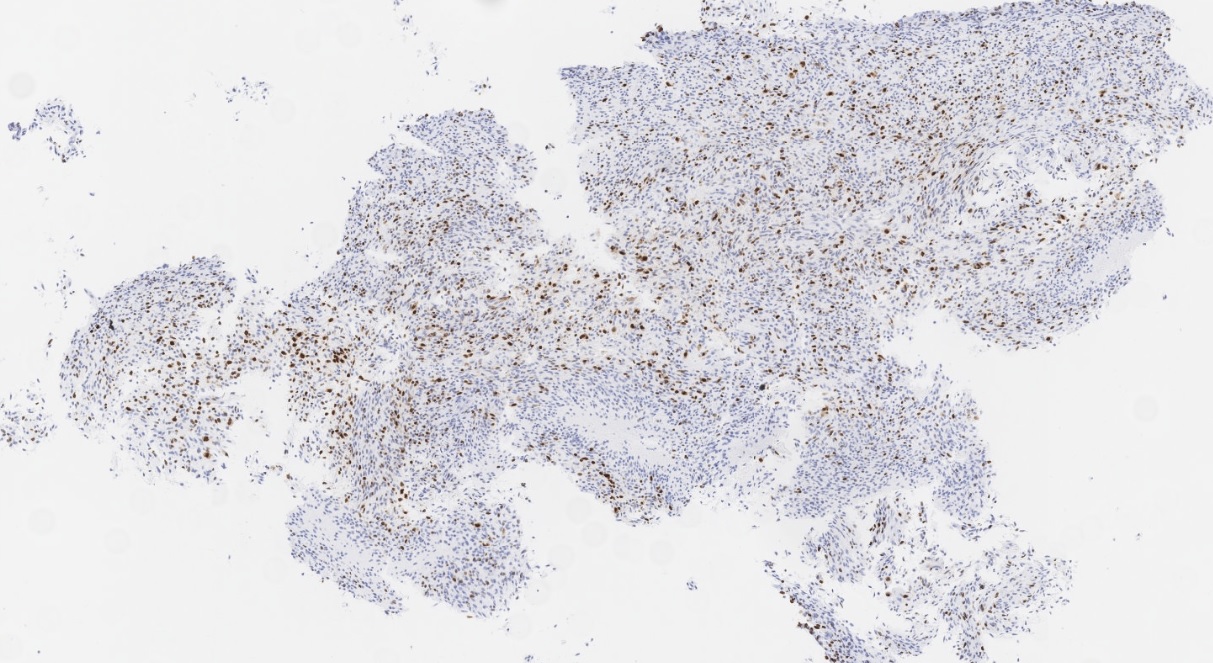
Figure 7 - P53 immunohistochemistry showing positivity in about 10% of tumor cells. (100X magnification)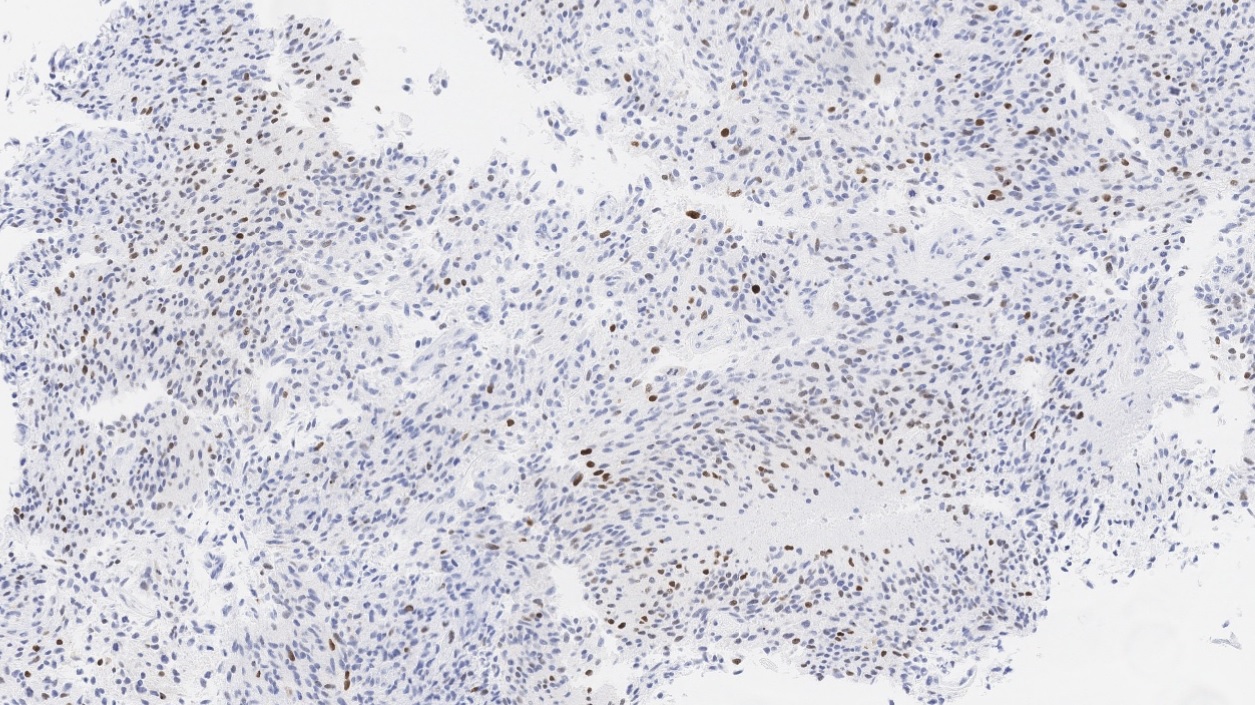
Molecular findings to-date of article originally published:
EGFRvIII Expression: Not Detected
EGFR amplification by FISH: Negative
Additional pending Molecular testing:
PTEN deletion (by FISH)
TERT promoter mutation by PCR
Tissue was insufficient for MGMT methylation testing.
What is the most likely diagnosis for her brain mass?
Choose one answer and submit.
 Meet our Residency Program Director
Meet our Residency Program Director