
Resident Program - Case of the Month
July 2019 - Presented by Ying Liu (Mentored by Anthony Karnezis)
Clinical History
Patient is a 71-year-old woman with persistent lower left quadrant pain and a CT scan that showed a solid 4 cm right ovarian mass. No extraovarian masses, ascites, or pleural effusion were noted. Family history was concerning for multiple relatives with breast cancer and a daughter who died in her early 30s from metastatic colon cancer.
Pathology Review:
Gross examination showed a circumscribed, ovoid, firm, rubbery yellow-tan mass with a pale-tan cut surface (3.9 x 2.6 x 1.4 cm) in the right ovary, which was submitted for frozen section analysis. Microscopic examination revealed a hypocellular spindle cell tumor growing in storiform and fascicular patterns. The cells contained bland, ovoid, tapered fusiform nuclei with eosinophilic cytoplasm that blended with a variable amounts of extracellular collagen. A diagnosis of fibroma was rendered. The patient underwent bilateral salpingo-oophorectomy; the contralateral ovary contained a similar mass (1.7 x 1.7 x 1.3 cm). No calcifications were observed in either ovarian mass.
Images:
(Click image to enlarge)

Figure 1: Right ovarian mass and fallopian tube

Figure 2: Left ovarian mass and multicystic ovarian parenchyma
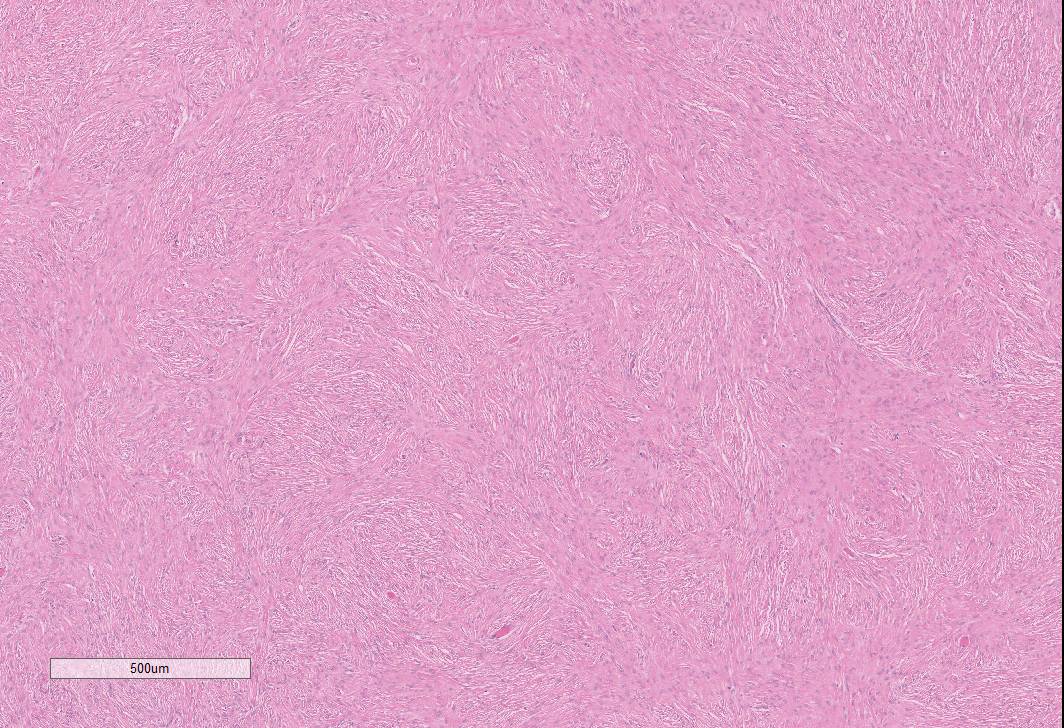
Figure 3: Ovarian fibroma, 4x
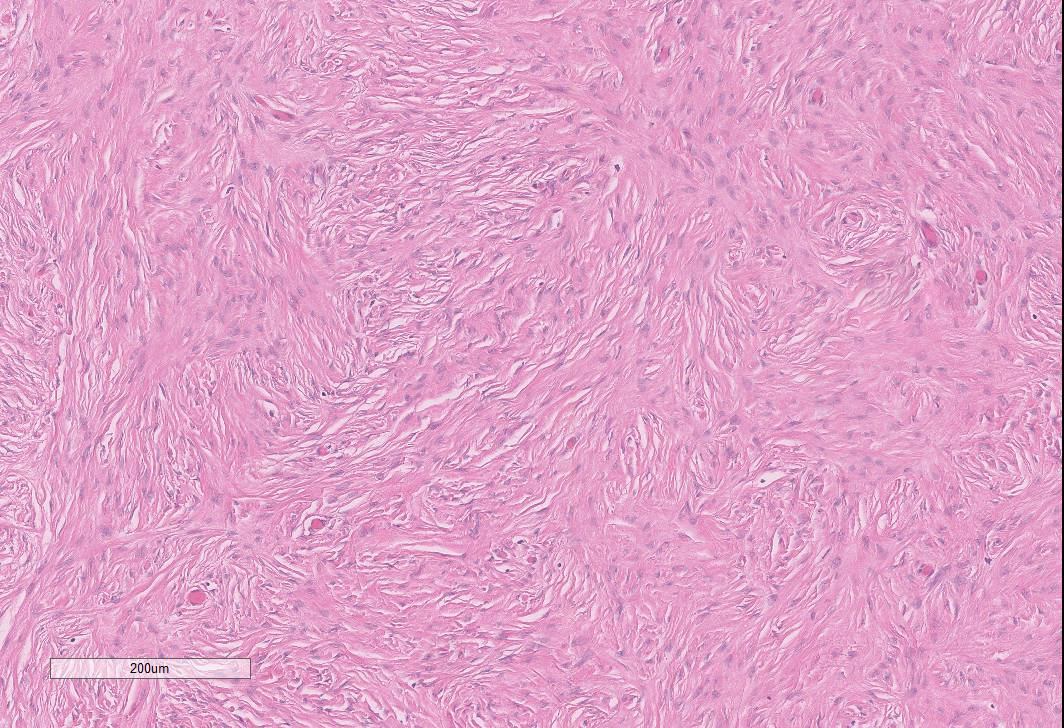
Figure 4: Ovarian fibroma, 10x
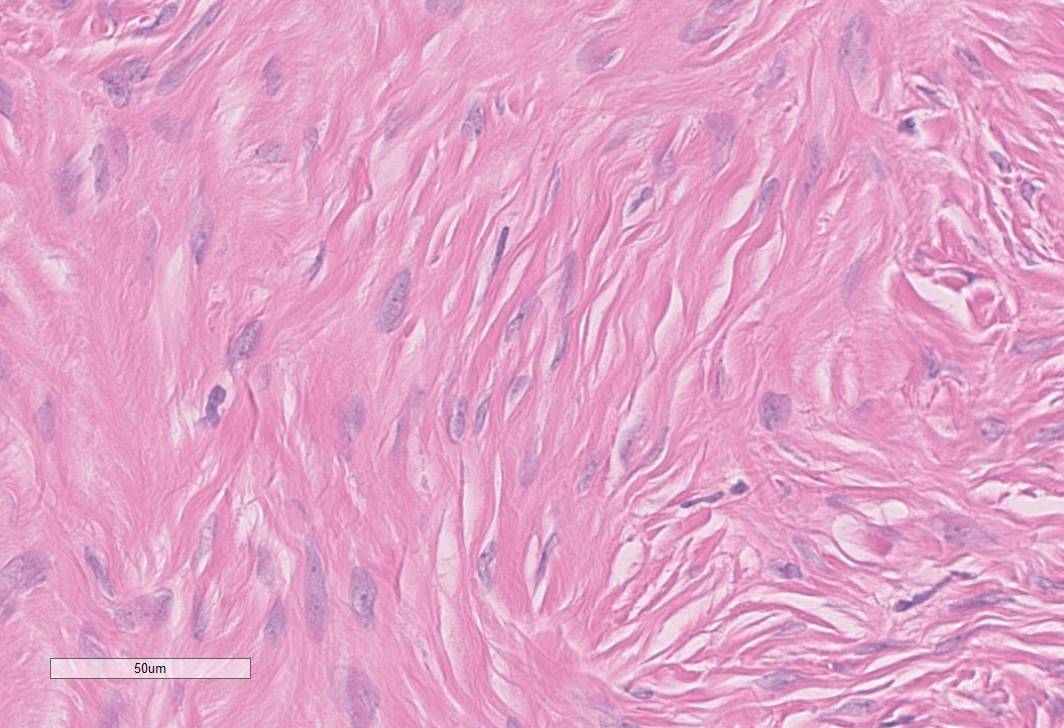
Figure 5: Ovarian fibroma, 40x
What syndrome is most often associated with bilateral fibromas?
Choose one answer and submit.
A.) Nevoid basal cell carcinoma syndrome
Ovarian fibromas constitute 5% of ovarian neoplasms, with an average age of onset of 48 years. More than 90% of cases are unilateral. Approximately 8% are bilateral and primarily associated with nevoid basal cell carcinoma syndrome (NBCCS, also known as Gorlin syndrome), a rare autosomal dominant disease estimated to affect 1 in 30,000 individuals.
> Learn more about this diagnosis.
 Meet our Residency Program Director
Meet our Residency Program Director