
April 2020 - Presented by Jacob Donnelly (Mentored by Joan Bernard)
Clinical History
A 77-year-old male presented to the hospital with gross hematuria. The patient has a history of benign prostatic hyperplasia (BPH) with outflow obstruction and had an elevated prostate specific antigen (PSA) in September of 2013 of 20.2 ng/mL (H). He underwent a cystoscopy with the following results:
The urethra was difficult to enter, but a small intraluminal papillary growth from the distal penile to mid bulbar urethra was identified.
The prostate had circumferential papillary growths starting proximal to verumontanum, approximately 2-3 cm in length. On retroflexion the intravesicular prostate appeared lobulated with a papillary mass identified.
The bladder had significant distention on entering and 350 mL of urine was aspirated.
No ureteral orifices on the right or left were seen.
No trabeculations were present.
The patient then underwent a urethral biopsy and transurethral resection of the prostate (TURP) procedure. The clinical impression was urothelial carcinoma.
Microscopic Findings
Initial H & E shows a predominantly papillary proliferation with relatively minimal stromal involvement. The papillae are lined by large cells with variably low and high N/C ratios, and the nuclei are round and have one or more prominent nucleoli. There is anisonucleosis.
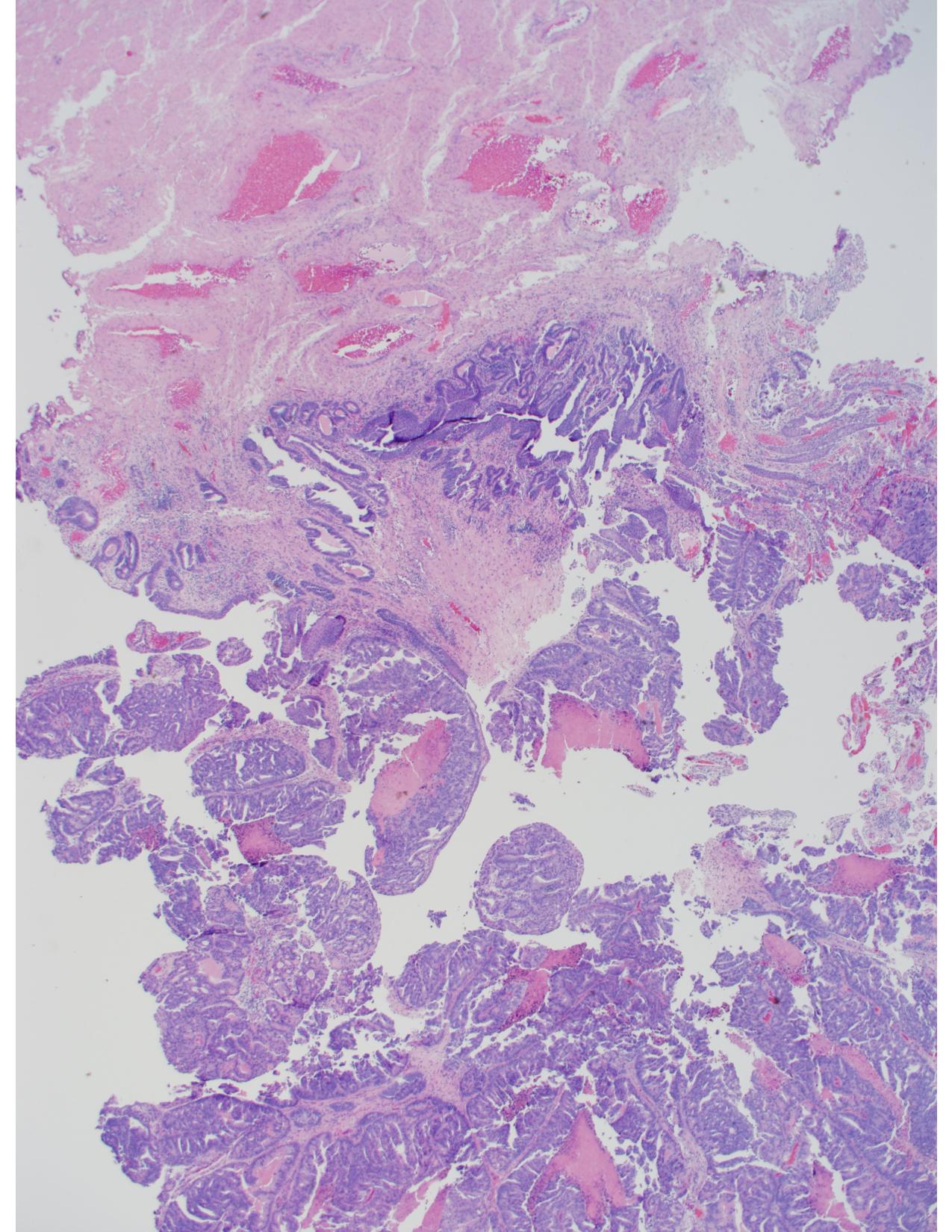
Figure 1. Prostatic Urethra 2X
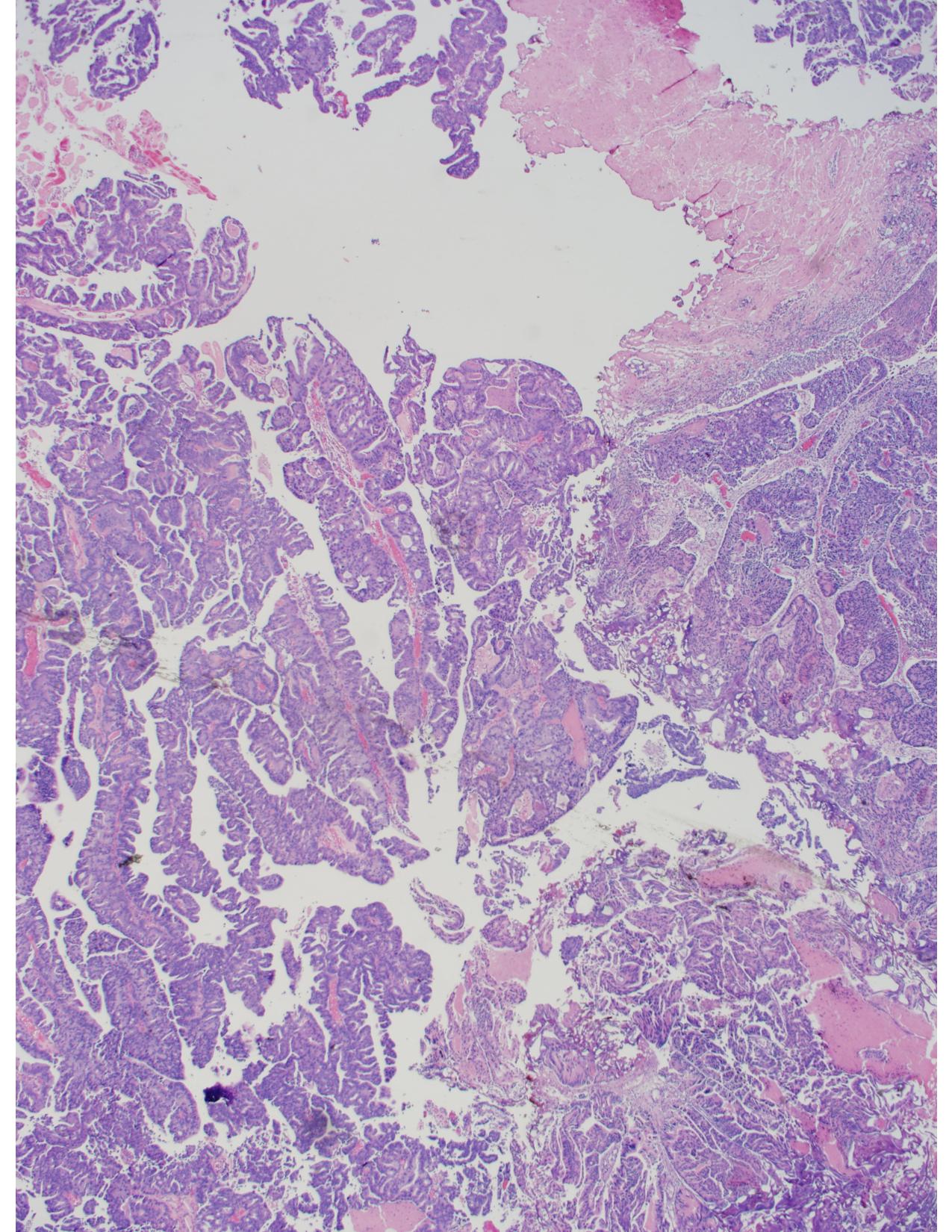
Figure 2. Prostatic Urethra Papillary Growth 2X
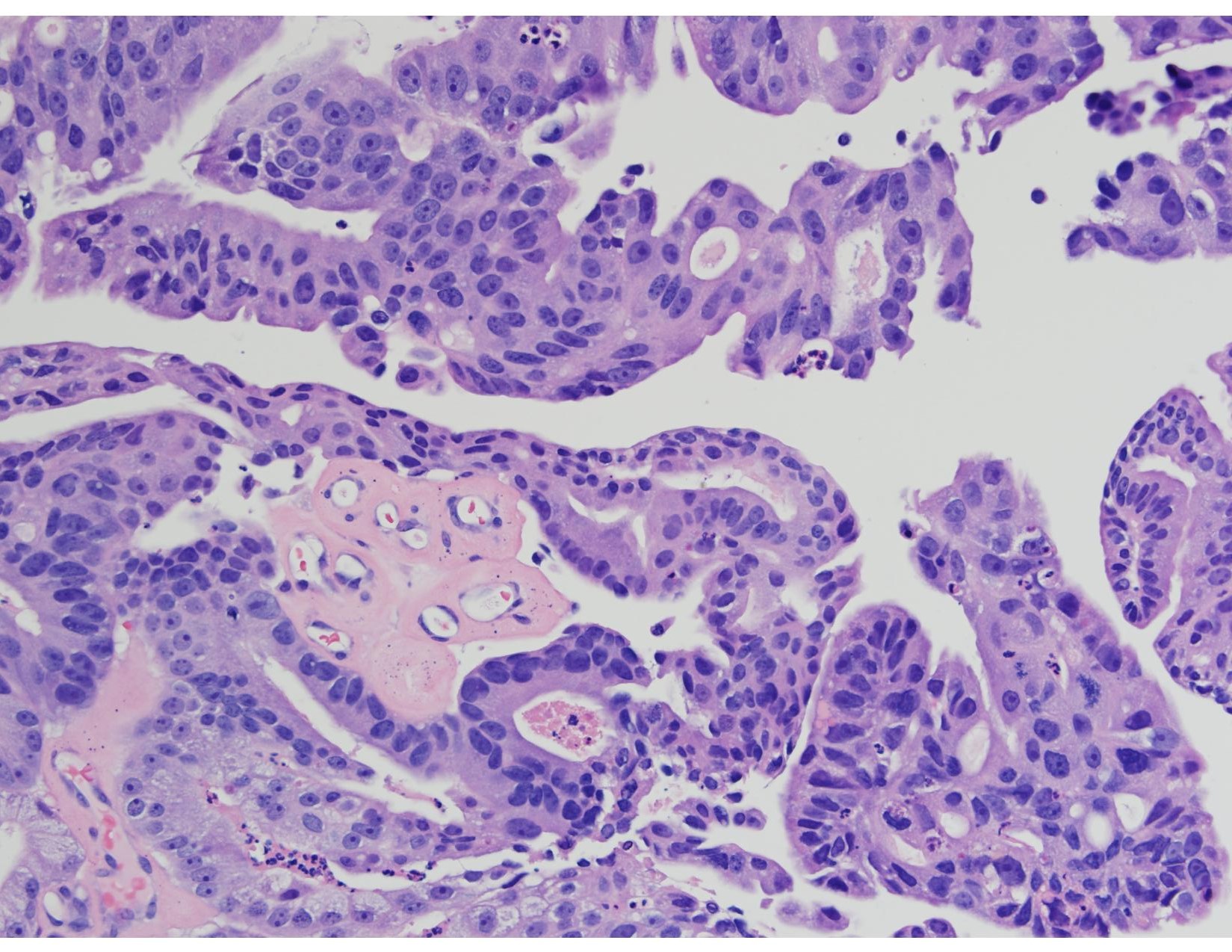
Figure 3. Prostatic Urethra 20X

Figure 4. CK7 Stain
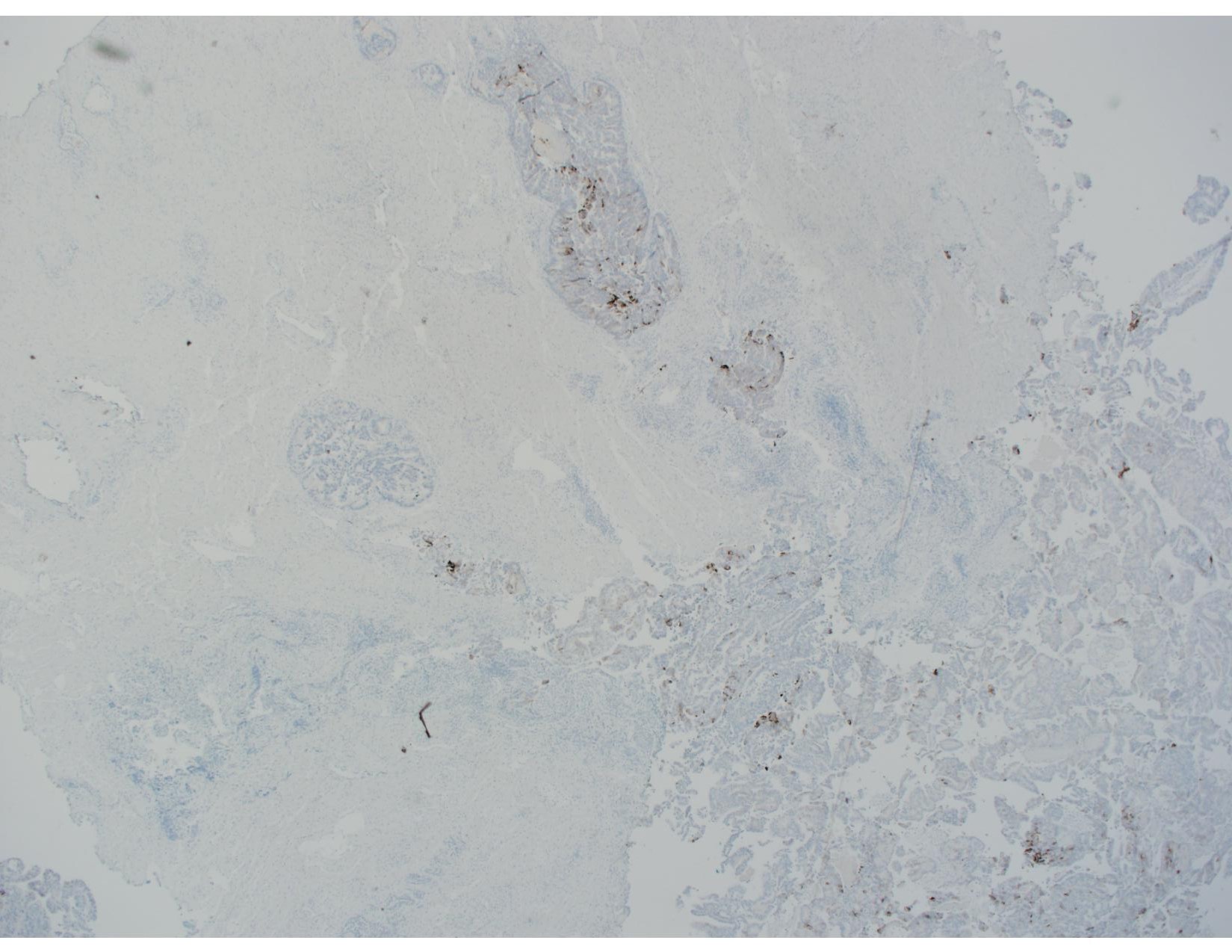
Figure 5. CK20 Stain

Figure 6. GATA3 Stain
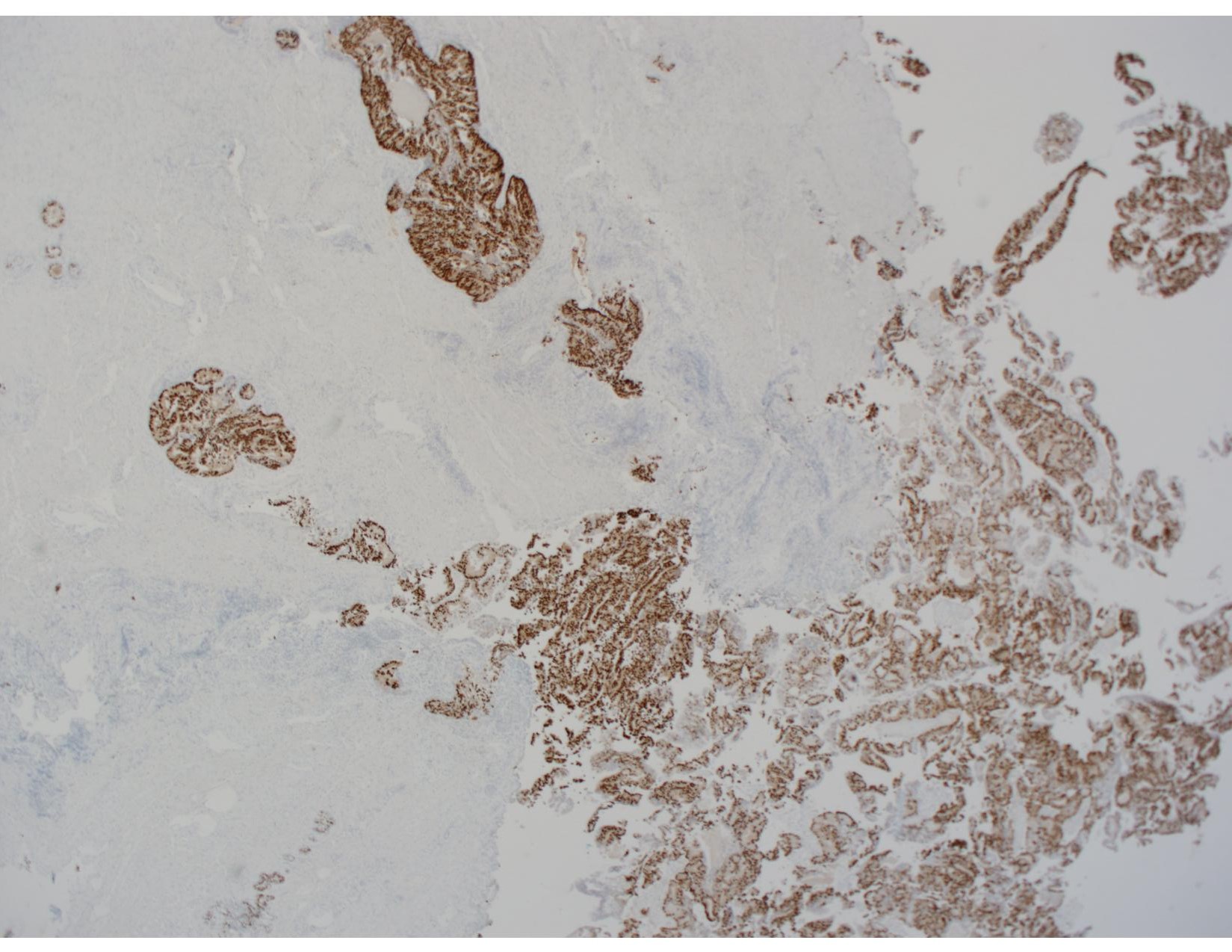
Figure 7. NKX3.1 Stain
Additional stains not pictured:
- PSA: Positive
- PSAP: Positive
 Meet our Residency Program Director
Meet our Residency Program Director