
December 2020 – Presented by Dr. Luke Dang (Mentored by Dr. Kurt Schaberg)
Clinical History:
A male in his early thirties with no significant past medical history presented with perineal pain several weeks after a ground level fall and was found to have a large peritoneal hematoma requiring drainage. A CT scan of the abdomen and pelvis demonstrated a large (14 x 13 x 8 cm), heterogeneously enhancing fluid collection which extended from the perineum to the base of the penis, with features suggestive of abscess superimposed on the known clinical history of trauma, with enlarged adjacent lymph nodes. The patient returned several days later to the emergency department with repeat bleeding. The patient was admitted before undergoing multiple procedures to control persistent bleeding from this site.
Macroscopic and microscopic description:
Fragments of red soft tissue from a debridement of this perineal wound were received for histopathologic examination. The specimen is primarily comprised of discohesive, large polygonal cells with abundant eosinophilic cytoplasm, eccentrically placed large atypical nuclei with vesicular chromatin, prominent nucleoli, and frequent mitoses (Figures 1-4). There is large amounts of adjacent hemorrhage and necrosis.
Ancillary Testing (Immunohistochemistry)
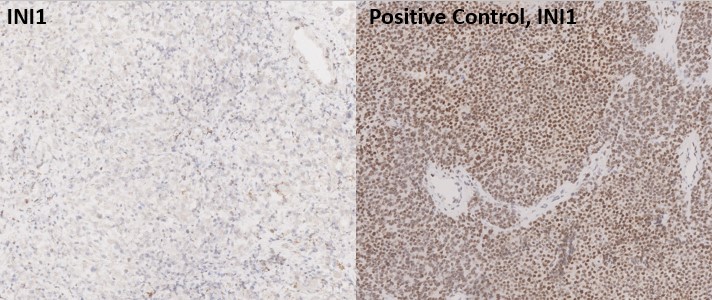
Tumor cells are strongly positive for AE1/AE3 (Figure 5), and negative for desmin, Sox-10, Melan-A, and OCT3/4. INI-1 loss is observed (Figure 6). CD138 stains scattered plasma cells.
Figure 1. H&E, low magnification (2x)
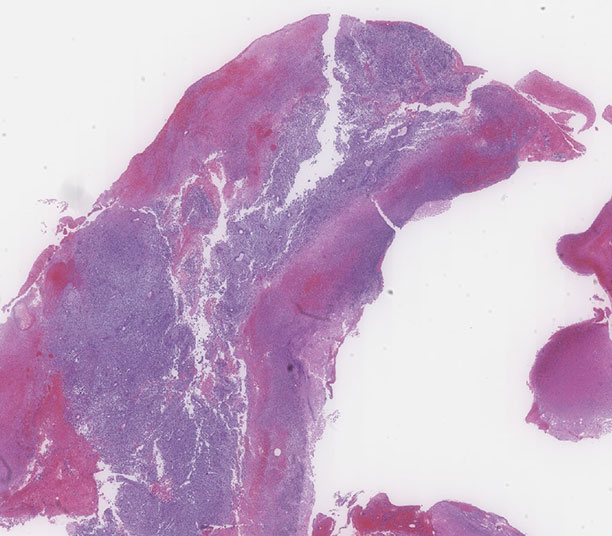
Figure 2. H&E, low magnification (5x)
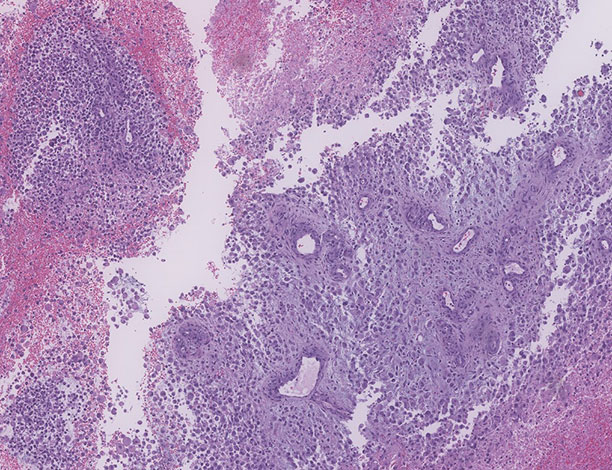
Figure 3. H&E, high magnification (20x)
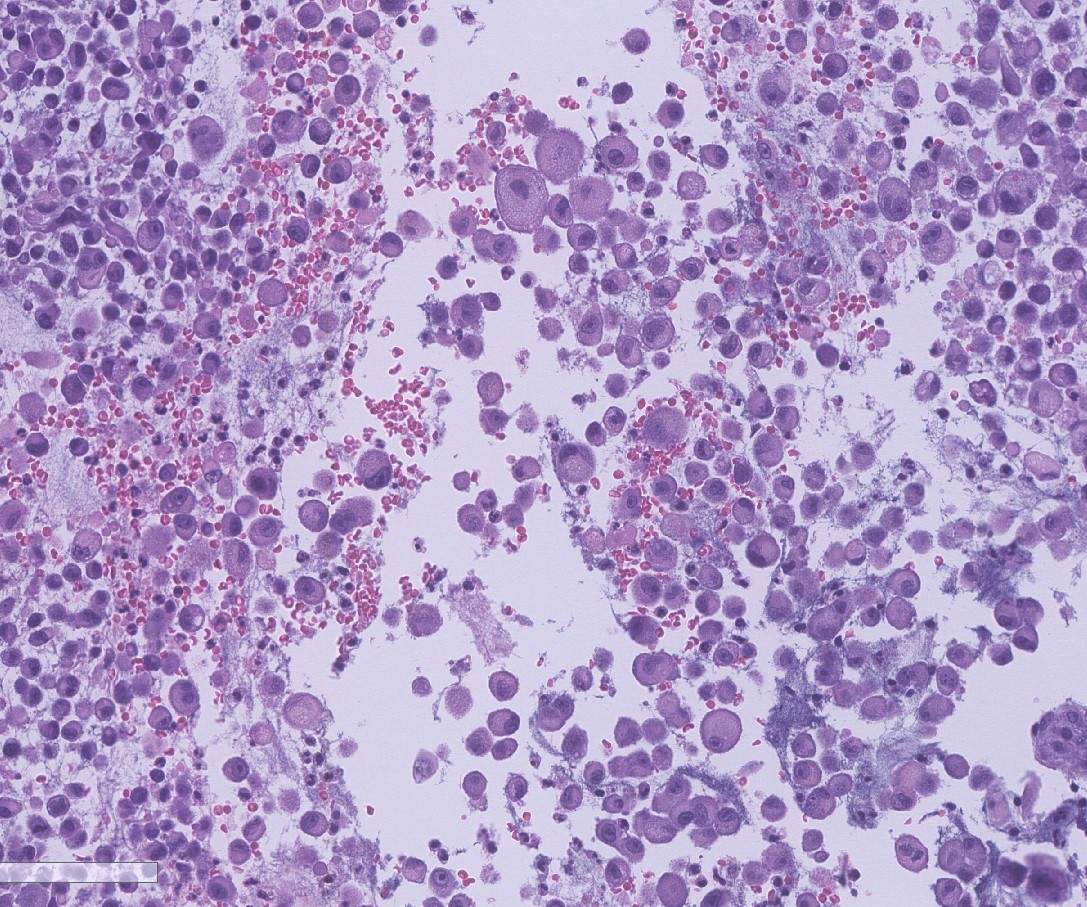
Figure 4. H&E, high magnification (40x)
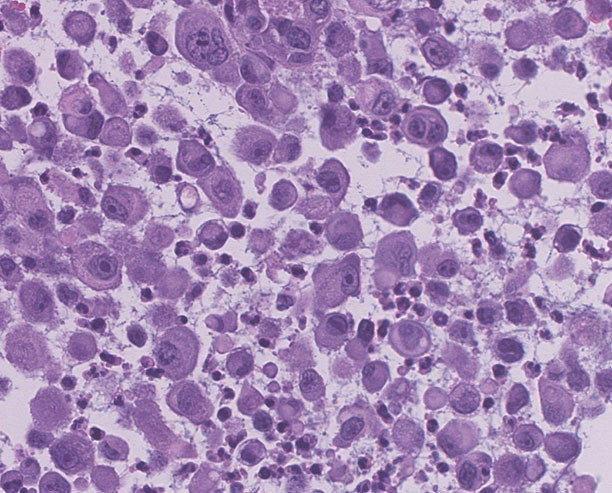
Figure 5. AE1/AE3 Immunohistochemical Stain (4X)
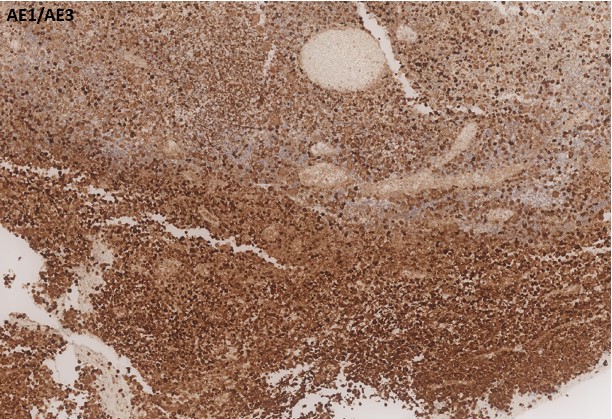
Figure 6. INI1 Immunohistochemical Stain (4X)
 Meet our Residency Program Director
Meet our Residency Program Director