
Resident Program - Case of the Month
April 2022 – Presented by Dr. Ahresh R. Saha (Mentored by Dr. Elham Betts)
Discussion
Hodgkin lymphoma is a type of lymphoma, in which Reed Sternberg cells are present. The presumption is that Reed-Sternberg cells derive from pre-apoptotic germinal center B cells.
Classical diagnostic Reed-Sternberg cells are large (15 to 45 micrometers), have abundant slightly basophilic or amphophilic cytoplasm and have at least two nuclear lobes or nuclei. Diagnostic Reed-Sternberg cells must have at least two nucleoli in two separate nuclear lobes.1
Reed-Sternberg cells are generally positive for CD15, CD30, and weak PAX5. They may be positive for MUM1, EBER, and PDL1/PDL2. They are generally negative for CD43, CD45, CD79a, BOB1, CD3, ALK1. In addition, they are generally negative for CD20 but may show variable expression and OCT2 is expressed in ~10% of the cases.2
There are four subtypes of Hodgkin’s lymphoma (nodular sclerosis, mixed cellularity, lymphocyte rich, lymphocyte depleted). The most common type is Nodular Sclerosis (~70% of Classical Hodgkin’s lymphoma in Western countries). It affects females more than males and is most common among the age 15 – 35-year age group. It primarily affects those in urban areas, wealthier nations and individuals with high socioeconomic status. In addition, it can be associated with EBV positivity (10 - 25%). The nodular sclerosis subtype exhibits nodularity, dense collagen bands, and a thickened lymph node capsule. Lacunar cells are also characteristic of the nodular sclerosis subtype and contain lobulated nuclei with pale retracted cytoplasm (artifact of formalin fixation), creating lacunae-like spaces. It can rarely affect the bone marrow, and this represents advanced disease.1
The differential diagnosis of Hodgkin’s lymphoma includes Diffuse Large B Cell Lymphoma (DLBCL) with anaplastic morphology and Anaplastic Large Cell Lymphoma (ALCL). DLBCL involves features such as large, transformed cells and Hodgkin’s/RS like cells. Immunohistochemistry is positive for the pan-B-cell antigens CD19, CD20, CD22, CD79a, and PAX5. Negative markers include CD10 and commonly BCL6. In addition, MUM1 and CD30 are frequently positive with coexpession of CD15. Anaplastic Large Cell Lymphoma may contain features such as sclerosis and eosinophil clusters, thereby mimicking Hodgkin’s lymphoma. In addition, in ALCL, the anaplastic cells are generally positive for CD30, but negative for CD15.
The following diagram shows Hodgkin’s lymphoma affecting the bone marrow with the immunohistochemical profile listed below.
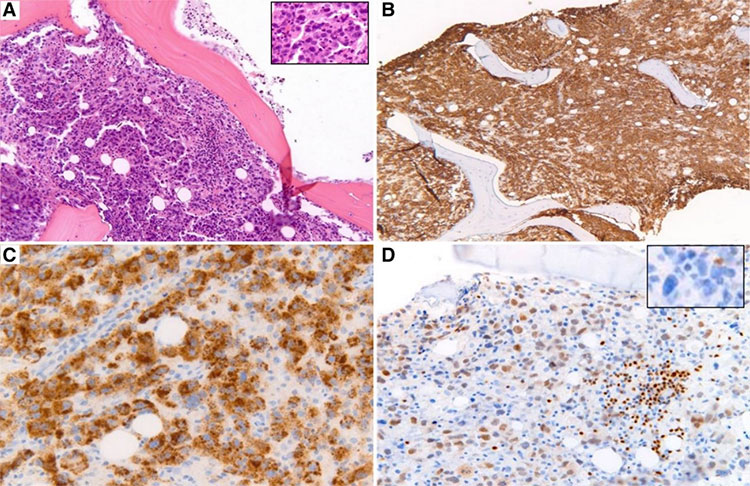
Primary bone marrow classic Hodgkin lymphoma (A) [hematoxylin and eosin (H&E)] [inset contains Hodgkin–Reed Sternberg (HRS) cells; H&E]. Tumor cells were strongly and diffusely positive for CD30 and CD15 (B,C, respectively). Tumor cells were weakly positive for PAX5 (D) and negative for CD20 (D).3
References
- Aggarwal P, Limaiem F. Reed Sternberg Cells. [Updated 2021 Jul 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
- MD, Edward C. Klatt. Hematopathology.
- Laurent, C., Arber, D.A., Johnston, P., Fend, F., Zamo, A. and Attygalle, A.D. (2020), Diagnosis of classic Hodgkin lymphoma on bone marrow biopsy. Histopathology, 76: 934-941.
- Swerdlow, Steven H. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. International Agency for Research on Cancer, 2017.
 Meet our Residency Program Director
Meet our Residency Program Director