
Resident Program - Case of the Month
August 2023 – Presented by Dr. Larry Ha (Presented at American Society for Clinical Pathology(ASCP))
Discussion
HPV-related multiphenotypic sinonasal carcinoma (HMSC) is a rare tumor that is restricted to the sinonasal tract, exhibits features of both a surface-derived and salivary gland carcinoma, and is associated with high-risk human papillomavirus (especially HPV 33) [1]. It has an indolent clinical behavior with frequent local recurrence in about 1/3 of patients but cervical lymph node metastasis is not identified and distant metastasis to lung and soft tissue is seen in about 5% of patients. HMSC is diagnosed mostly in patients 28- 90 years of age (mean of 54 years) with a slightly higher female predominance. This is a rare case of HMSC with an aggressive behavior with metastasis to the dura mater.
Microscopic examination revealed sections of carcinoma with various architectural patterns comprised of foci with adenoid cystic carcinoma-like morphology, basaloid squamous cell carcinoma and adenocarcinoma. The tumor showed positive immunostaining for P40, but focal reactivity to S100 and rare scattered reactivity with CD117. INI-1 was retained in tumor cells. P16 immunostain was strong and diffuse and high-risk cocktail HPV RNA ISH was positive. However, MYB FISH testing was equivocal. Morphologic and immunophenotypic findings were consistent with HMSC. The tumor involved the olfactory nerve fibers requiring a skull base resection and showed extension into the dura mater (see pictures below).
In a series of 49 cases [1], 43% of HMSCs initially presented with a T3 or T4 stage. In 38 cases where follow-up data was available, 14 recurred locally and 2 metastasized (lung and finger) but no reported regional lymph node metastasis or tumor-related deaths. Surgery of the primary tumor followed by radiation therapy for close or positive margins is the recommended treatment[1]. However, according to Bishop et al, routine lymph node dissection and chemotherapy do not appear to be indicated for HMSC since documented regional or distant disease has not been reported.
Diagnosis requires a mix of histologic features and clinical suspicion with the mainstay being multiple surface and salivary gland carcinoma components and positivity for HPV [3]. Appropriate radiological and pathologic correlation with good sampling is key to correctly stage the tumor in order to determine the next appropriate treatment.
In conclusion, HMSC presents as a large sinonasal mass with high-grade histologic features that is paradoxically indolent but this case shows a rare clinically aggressive behavior. Characteristic histologic and immunohistochemical features will aid in the diagnosis of HMSC. Surgical excision is highly recommended for treatment. When it invades locally and aggressively, treatment may require a skull base resection. In any case, patients require follow-up as local recurrence is common.
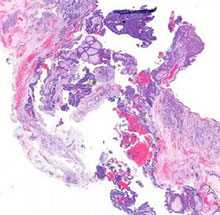 Invading Dura
Invading Dura
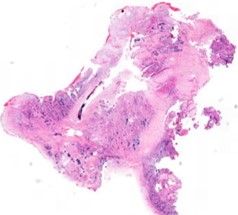 Invading Nerve
Invading Nerve
References
- Bishop JA, Andreasen S: "HPV-related Multiphenotypic Sinonasal Carcinoma: An Expanded Series of 49 Cases of the Tumor Formerly Known as HPV-related Carcinoma with Adenoid Cystic Carcinoma-Like Features". Am J Surg Pathol. 2017, 41(12):1690-1701. 10.1097/PAS.0000000000000944
- Rodarte AI, Parikh AS: "Human Papillomavirus Related Multiphenotypic Sinonasal Carcinoma: Report of a Case with Early and Progressive Metastatic Disease". J Neurol Surg Rep. 2019 Oct, 80(4):e41-e43. 1055/s-0039-3399571
- Jiromaru R, Yamamoto H: "HPV-related Sinonasal Carcinoma Clinicopathologic Features, Diagnostic Utility of p16 and Rb Immunohistochemistry, and EGFR Copy Number Alteration". The American Journal of Surgical Pathology: 2020 Mar, 44(3): 305-315. 10.1097/PAS.0000000000001410
 Meet our Residency Program Director
Meet our Residency Program Director