
Residency Program - Case of the Month
November 2012 - Presented by Kali Tu, M.D.
Clinical history:
The patient is a 27yr old male with a recent history of recurrent pneumonia (5 times over the past two years). Each episode of pneumonia was diagnosed and treated in ER but reportedly no convalescent chest radiograph was ever performed. The patient has a history of smoking cigarettes 1.5 PPD x 2 yrs and quite in 2011. He complains of a chronic cough productive of green sputum and blood up to a teaspoon, right sided chest pain that is constant and increases with cough, low grade fevers, night sweats, anorexia, weight loss, nocturnal cough, dyspnea at rest, dyspnea on exertion but can walk long distances, fatigue, malaise, and wheezing. The patient has been exposed to tuberculosis, but has had negative PPDs. There is no asbestos exposure, weight gain, anginal chest pain, pedal edema.
Work up:
A chest CT scan from an outside hospital shows a right main bronchus tumor with subtotal occlusion, right upper lobe collapse, and mediastinal adenopathy.
The patient has had previous bronchoscopies (at an outside hospital) which were nondiagnostic. He presents to UC Davis for further evaluation.
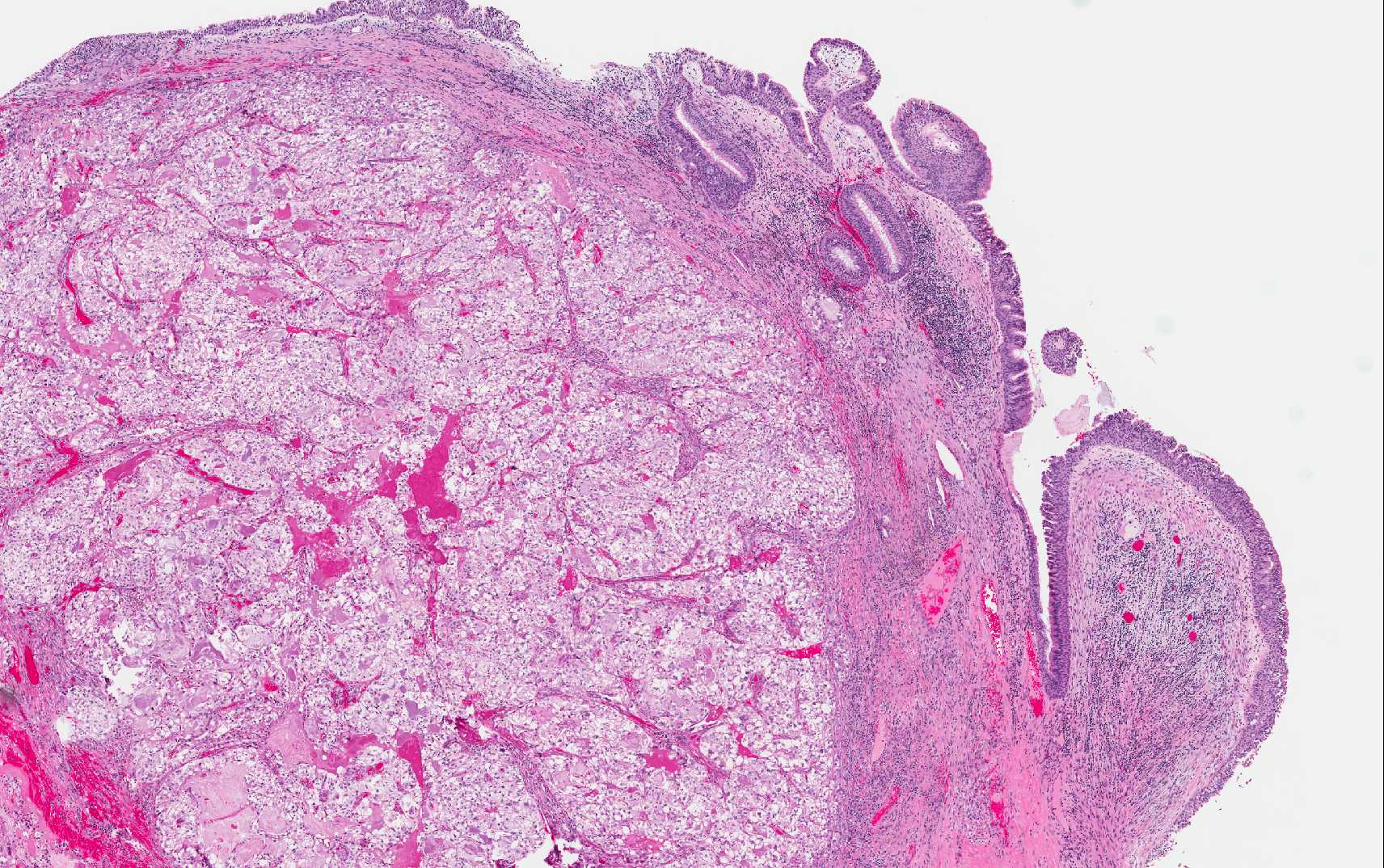
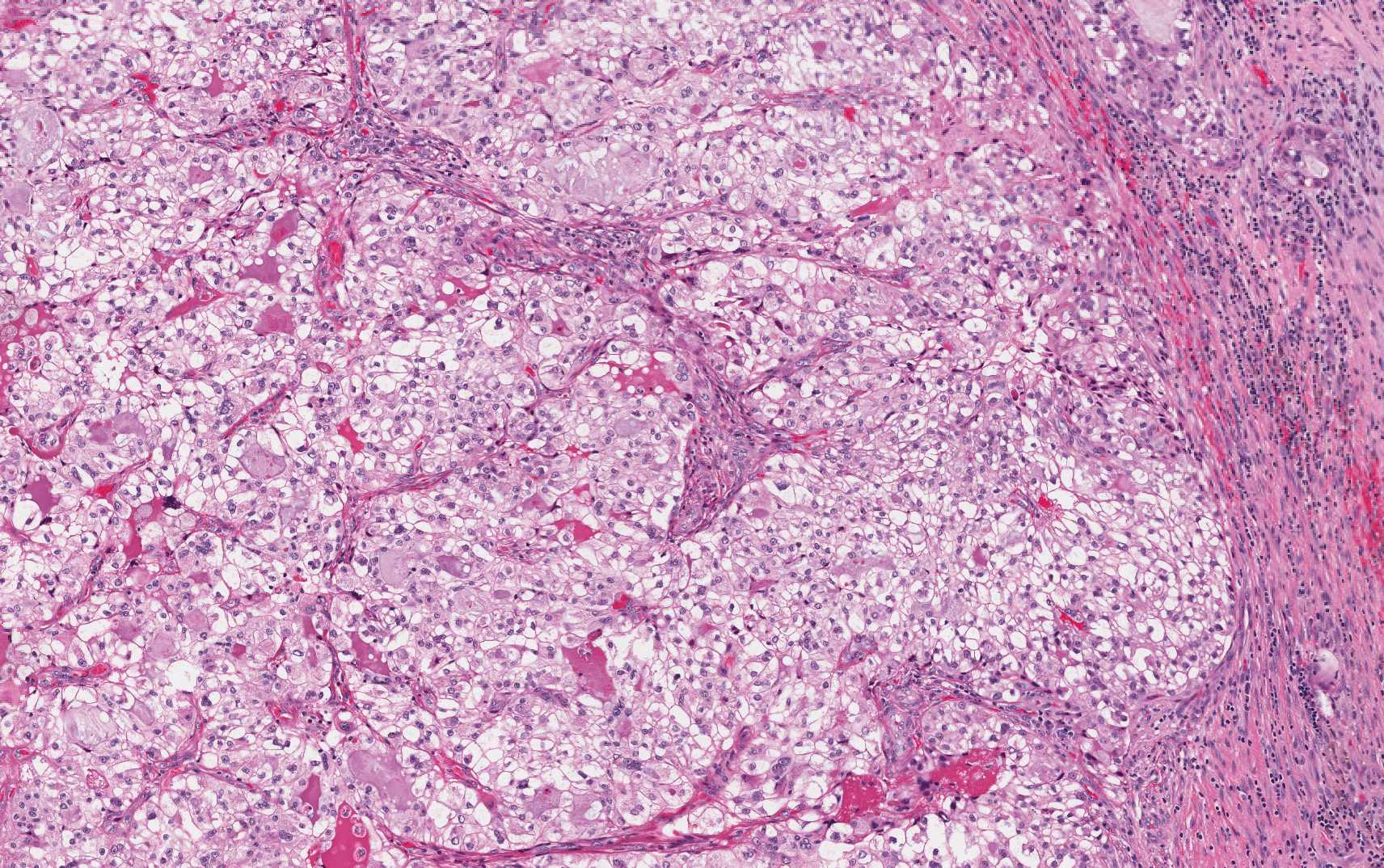
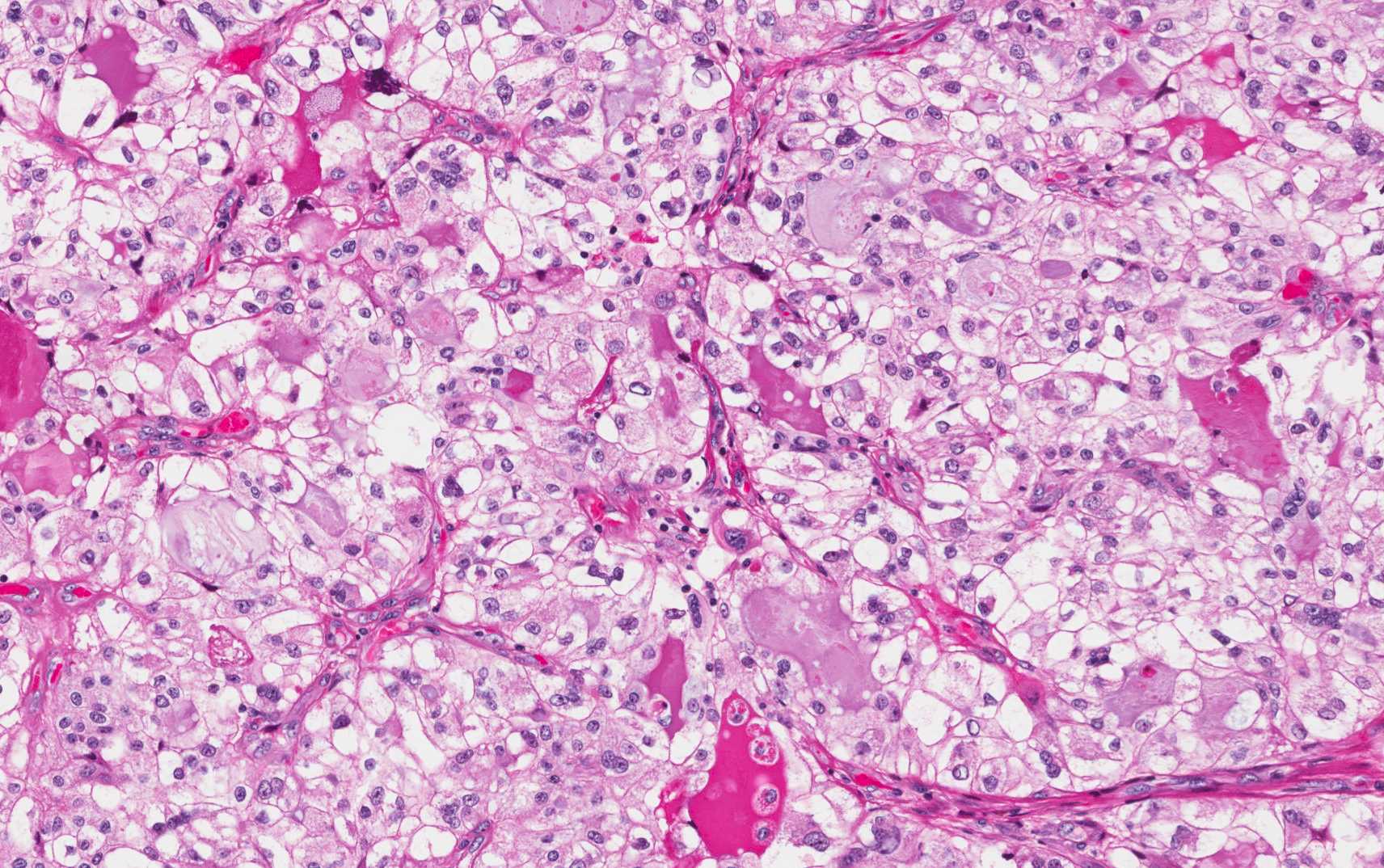
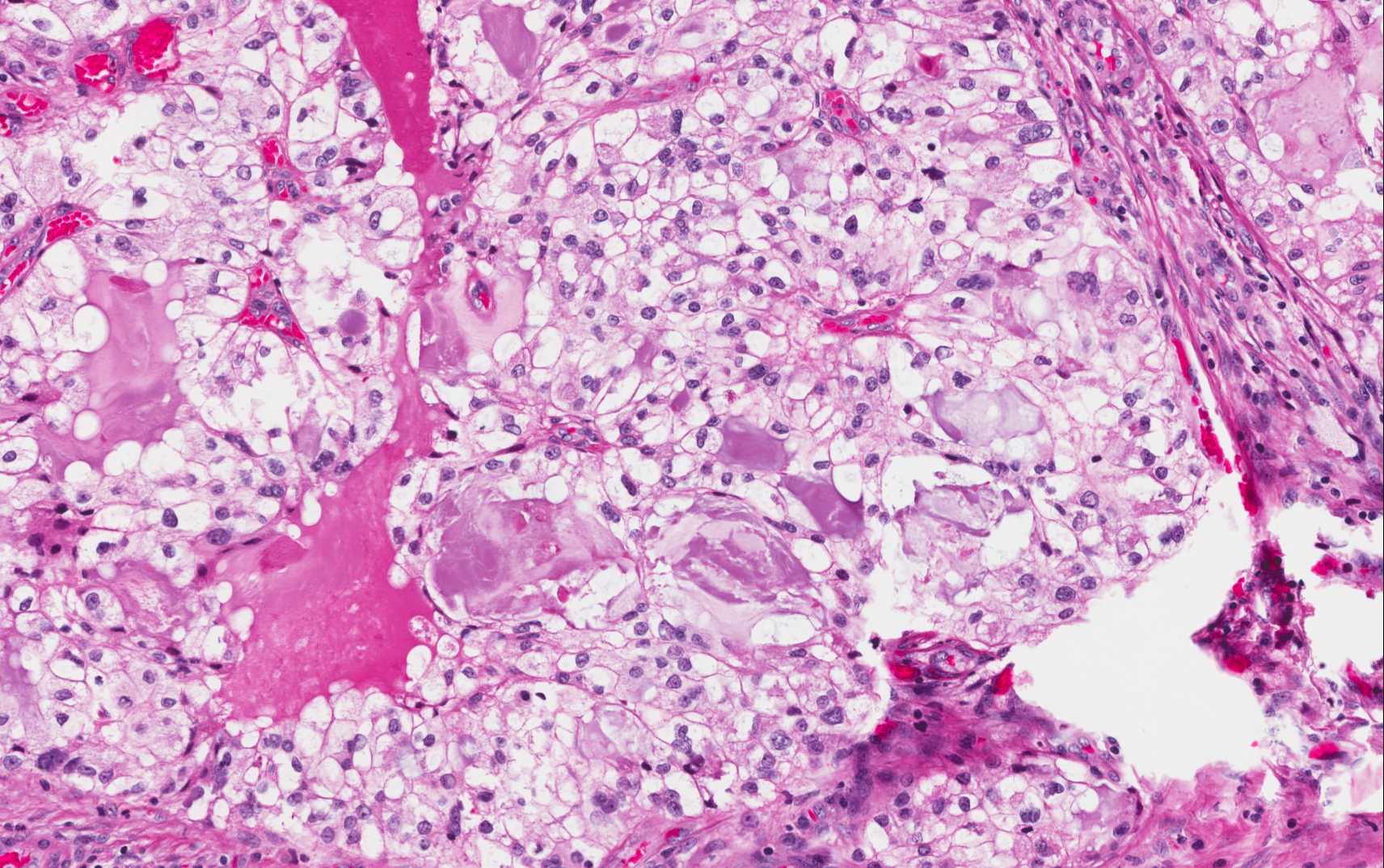
A bronchoscopy was performed which identified a tumor in the proximal right main bronchus occluding the bronchus. The tumor appeared to emanate from the right upper lobe and extend down the right bronchus intermedius posteriorly and laterally. The distal right bronchus intermedius was free of tumor but inflamed and erythematous. Biopsies were taken for routine pathology
Images:
 |
 |
 |
 |
Special stains:
|
CK5 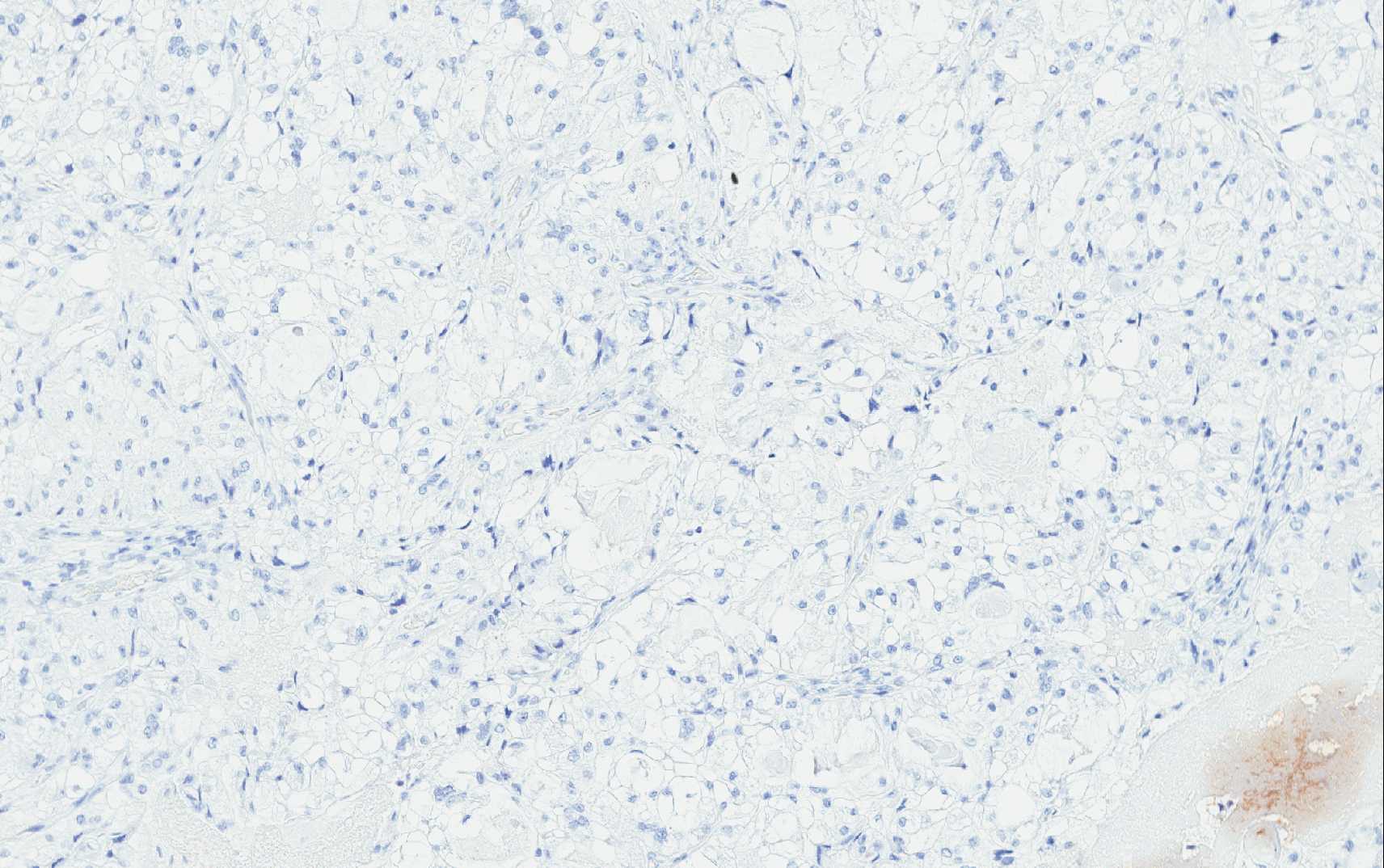 |
CK7 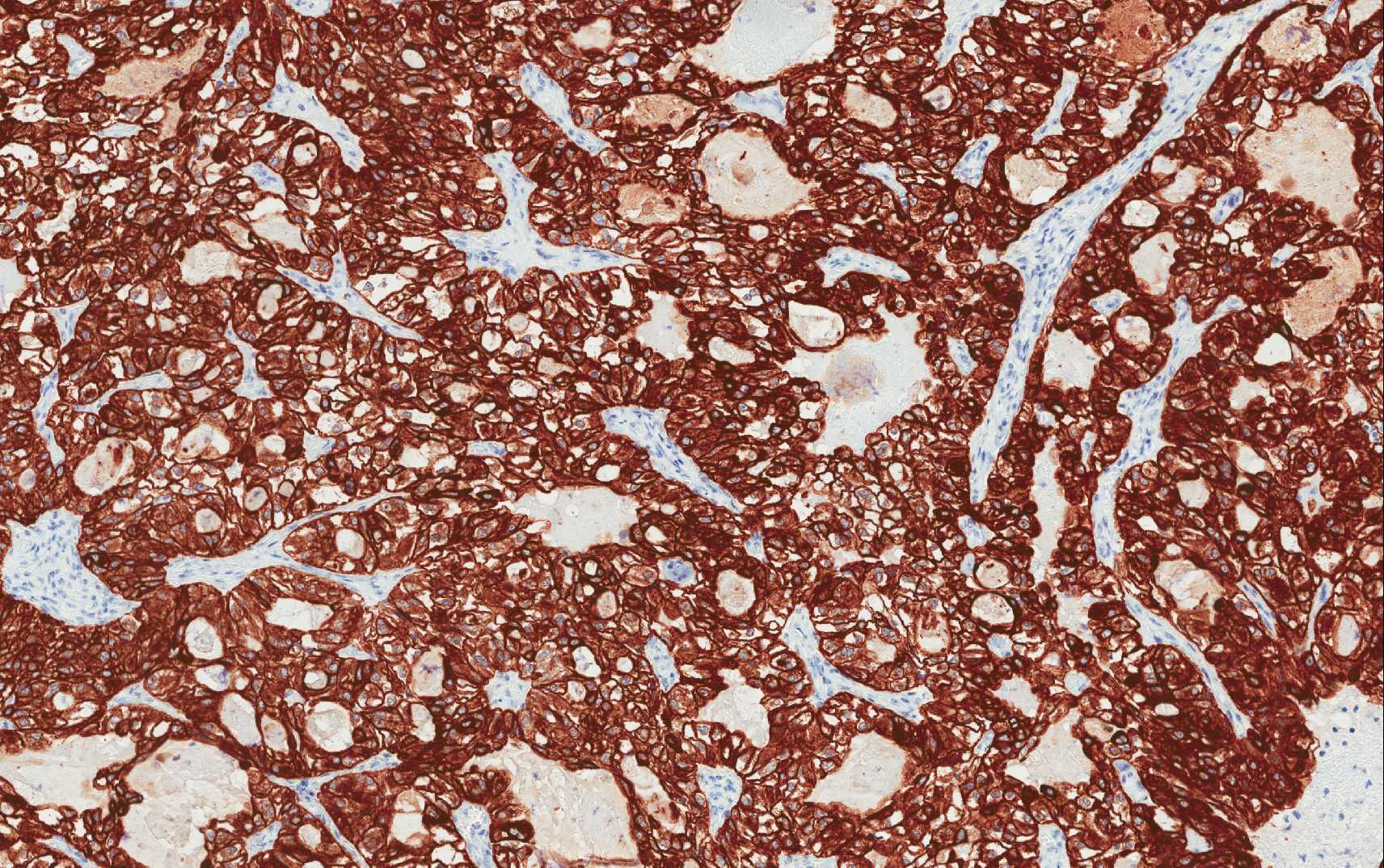 |
HMB45 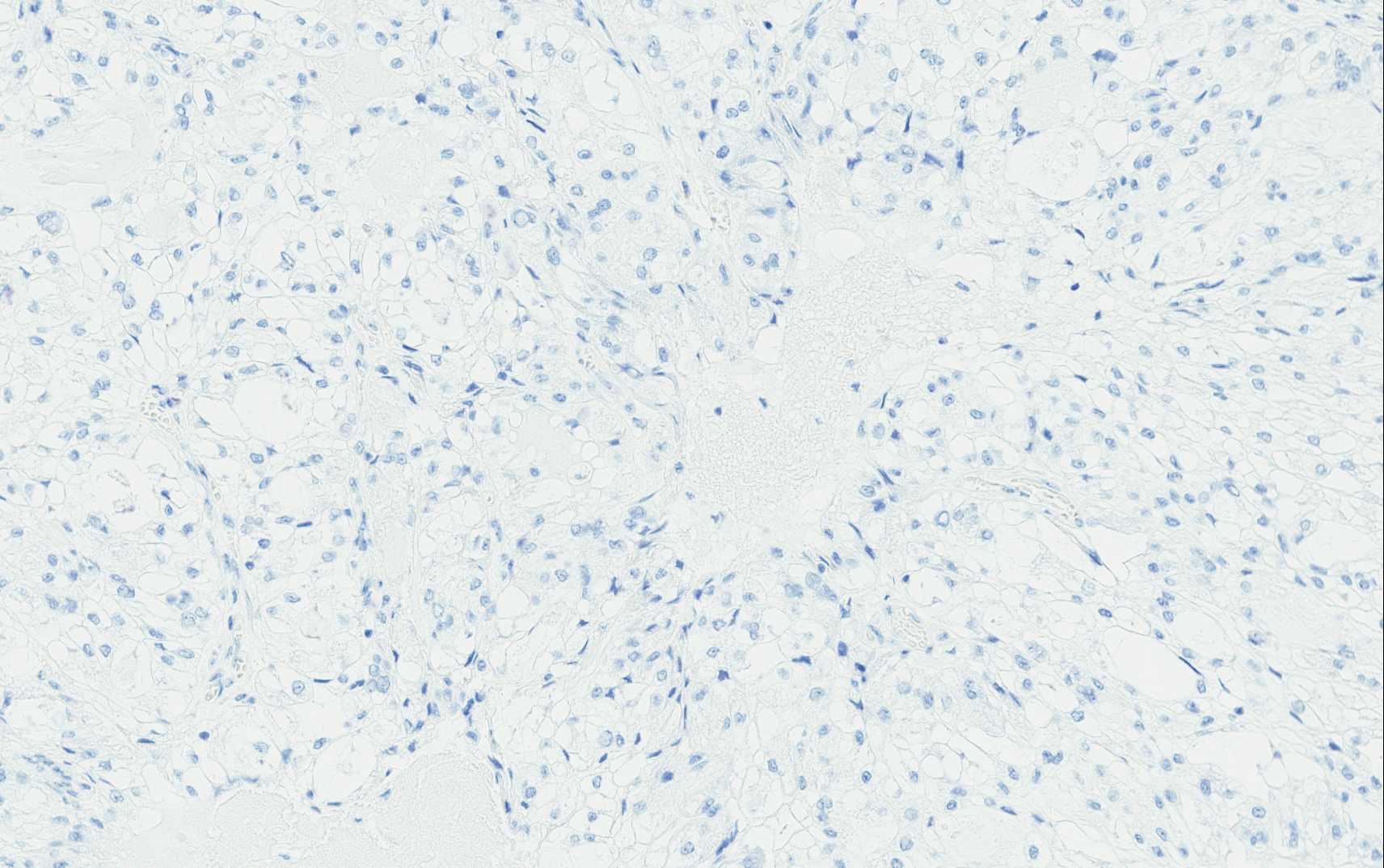 |
||
|
NapsinA 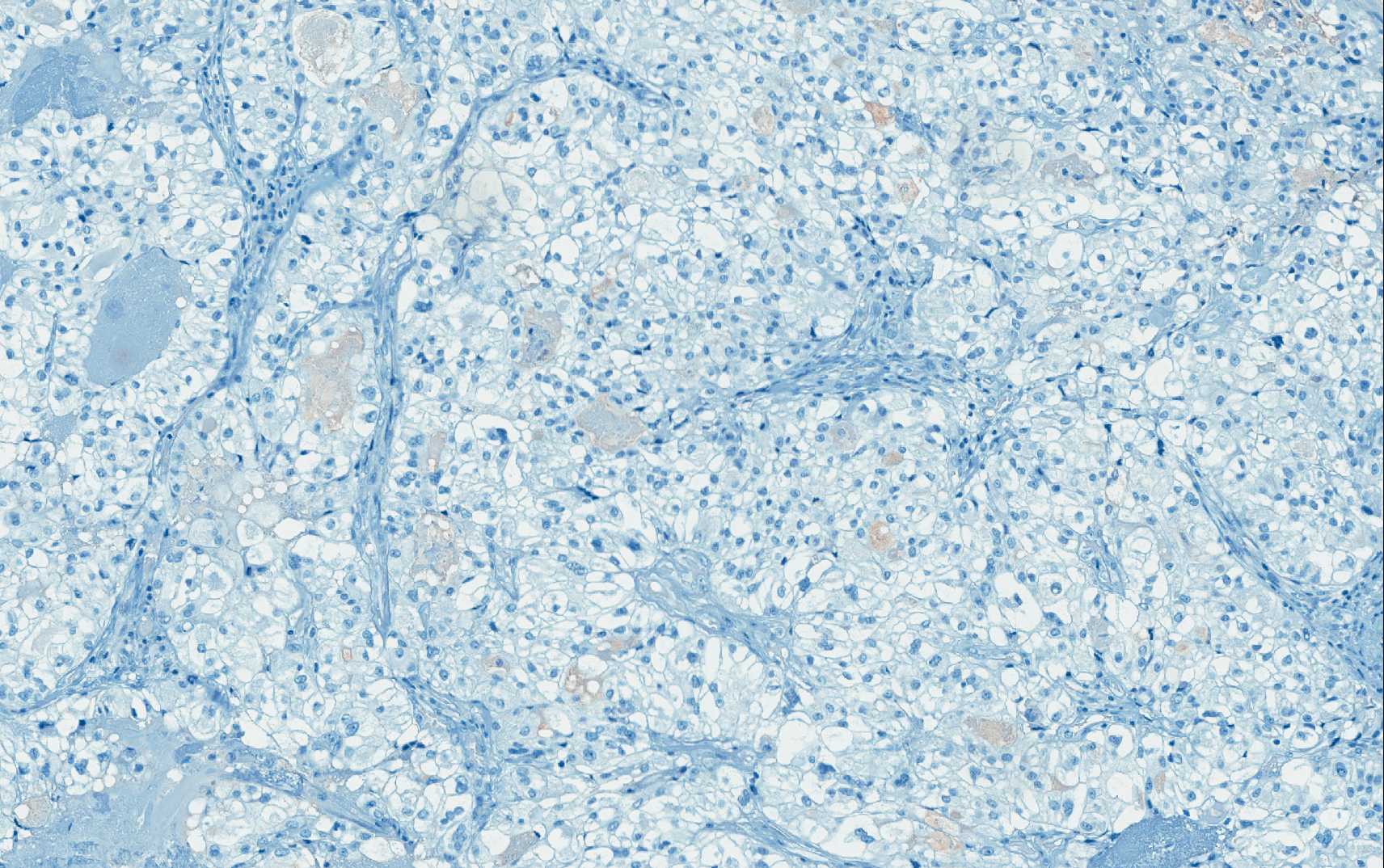 |
pas 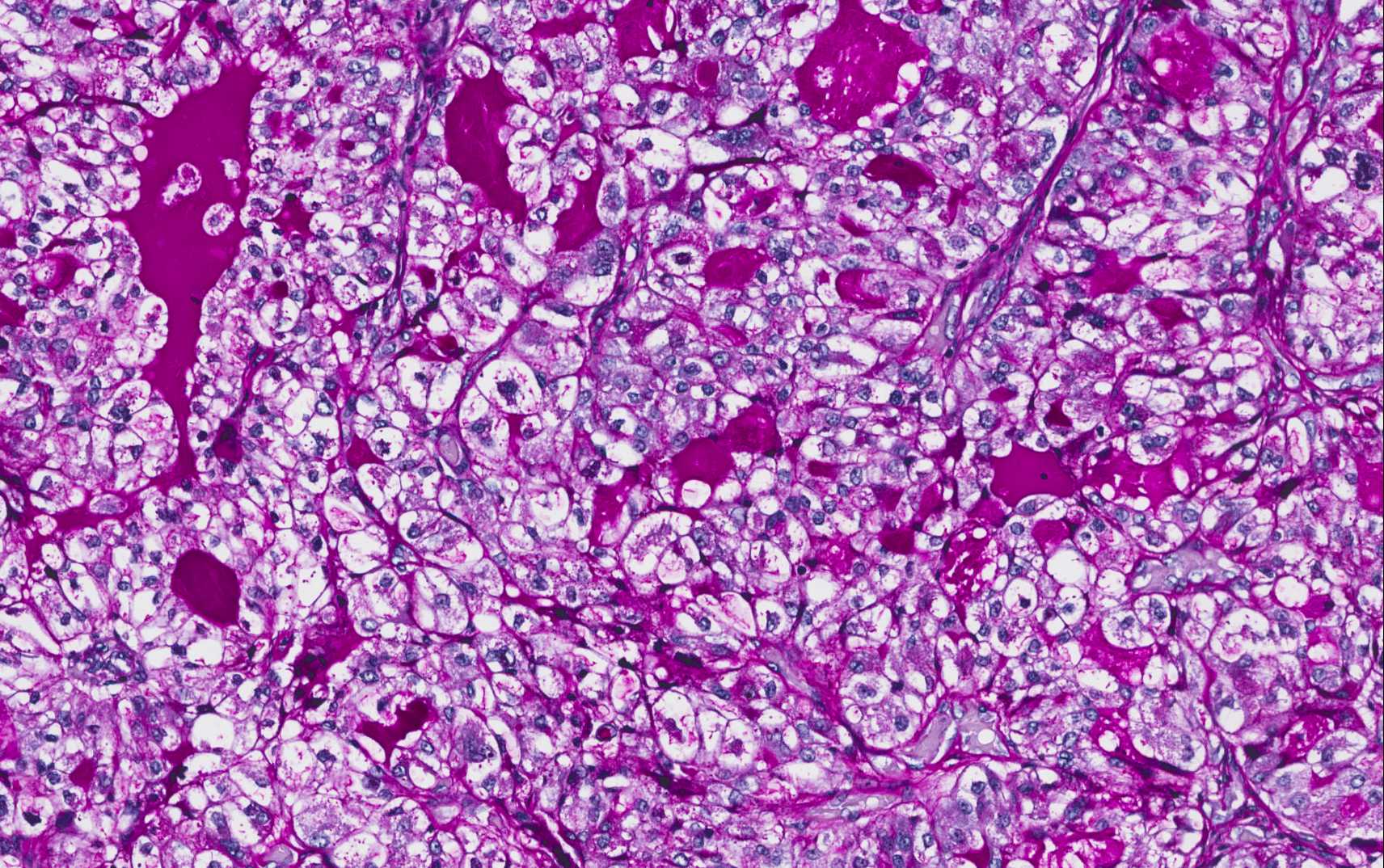 |
pasD 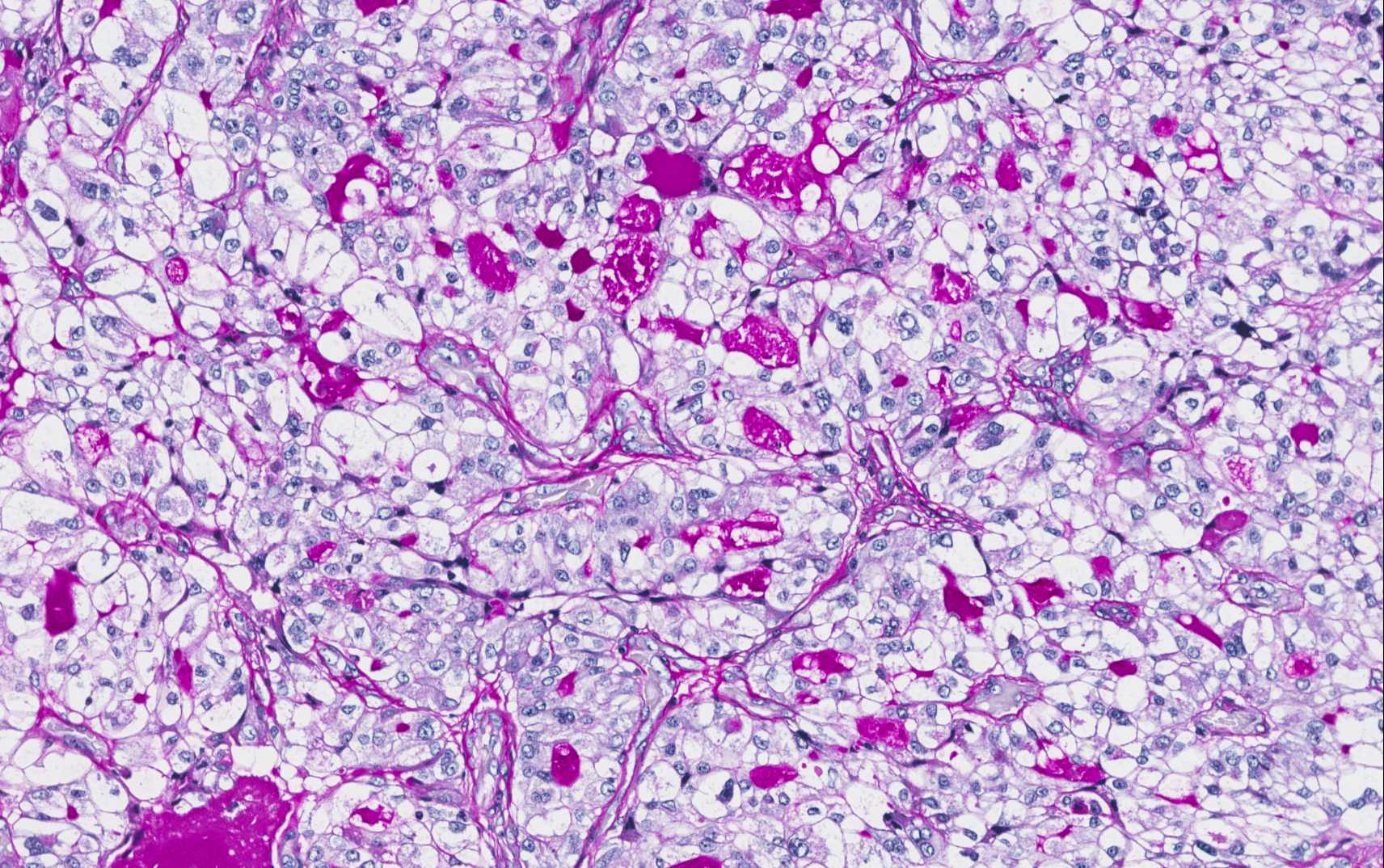 |
||
|
p63 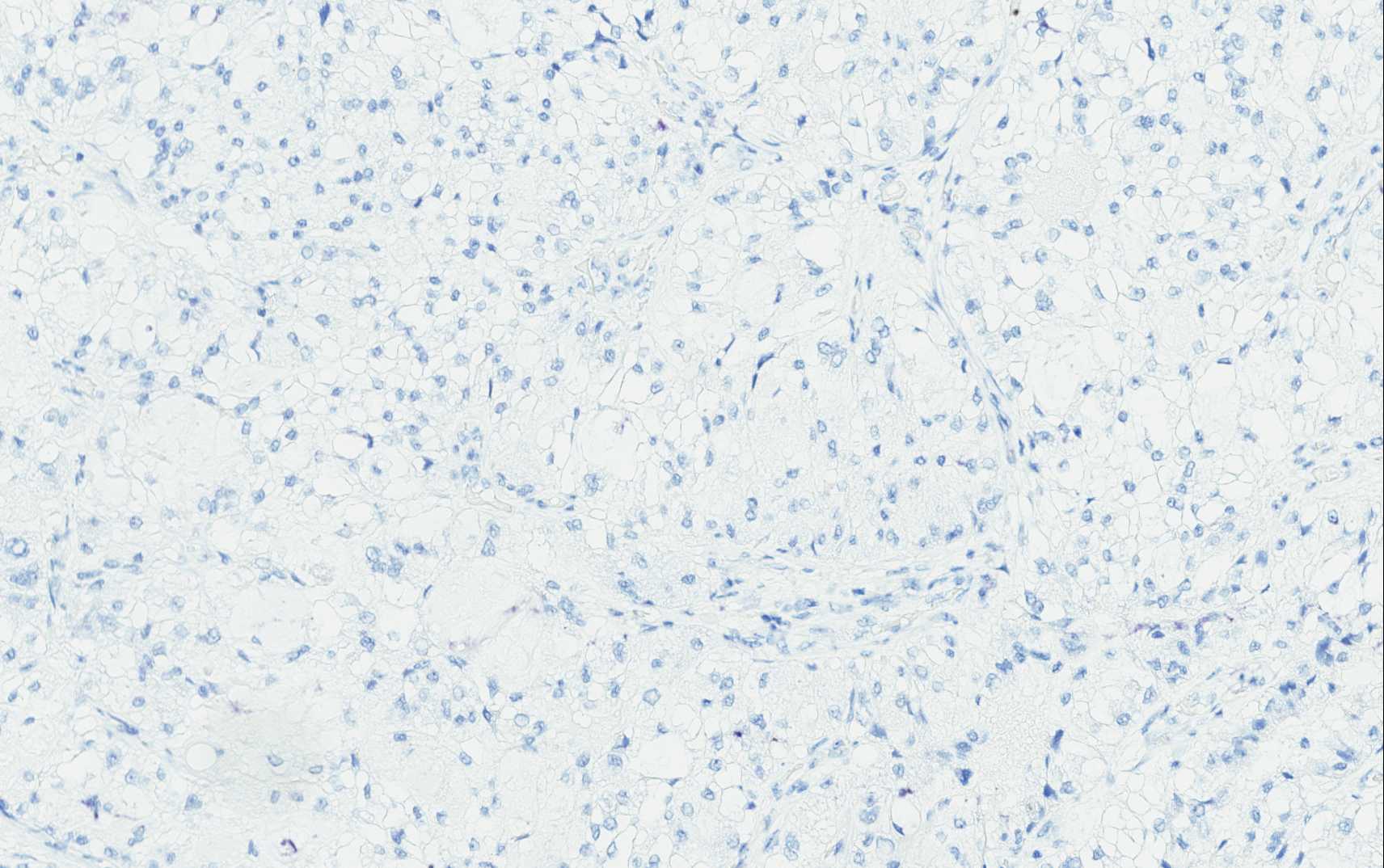 |
RCC 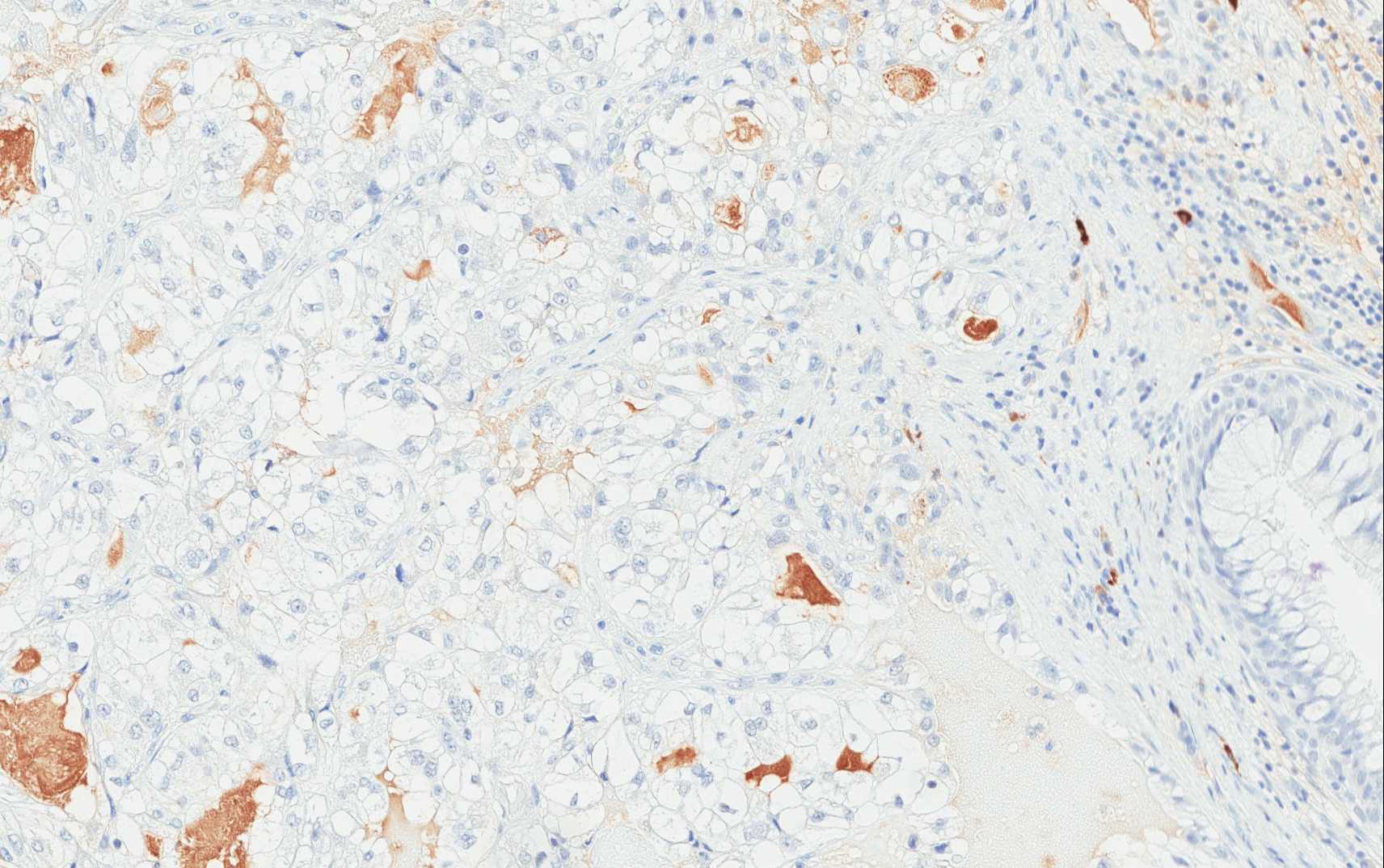 |
TTF1  |
 Meet our Residency Program Director
Meet our Residency Program Director