
Residency Program - Case of the Month
July 2016 - Presented by Jessica Rogers and Eric Huang
Clinical History
A 46-year-old G2P2 female presented with bleeding and cramping pelvic pain that had gradually gotten worse. She complained of spotting in between her periods with clotting every six months. She had been experiencing dizziness for about a month. She denied any other vaginal discharge. No change in bowel or bladder function and no fever or chills. The patient underwent endocervical curettage that showed adenocarcinoma.
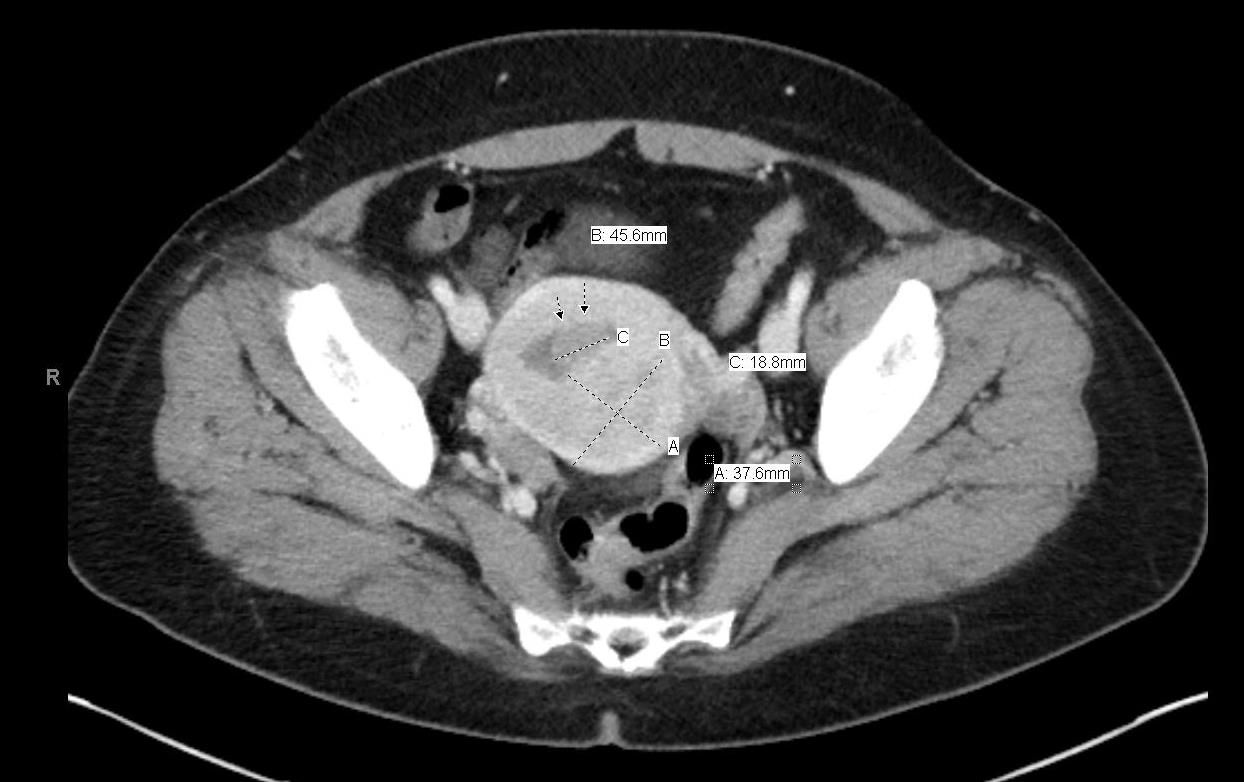
Even though the adenocarcinoma was seen on an endocervical specimen, imaging revealed a 1.1 x 1.7 x 1.9 cm endometrial mass, which radiology called “consistent with the known diagnosis of adenocarcinoma” as well as a second 4.9 x 4.1 cm mass arising in the posterior uterine wall that “directly abuts the endometrial finding”. Per radiology, this second mass was favored to be a leiomyoma with local extension of the endometrial tumor possible but less likely.
Click image to enlarge.
Gross
A 204g uterus was received with an 8mm polyp at the cervical os. The endometrium show a 5.7 cm fleshy, fairly well demarcated, trabeculated pink to tan tumor mass posteriorly that extended into the myometrium. The gross photo shows a cross section through the posterior wall endometrial mass, which is separate from the endocervical polyp (not shown).
Click image to enlarge.

Microscopic
Islands of tumor cells that permeate the myometrium with “tongue-like” growth.
Click images to enlarge.
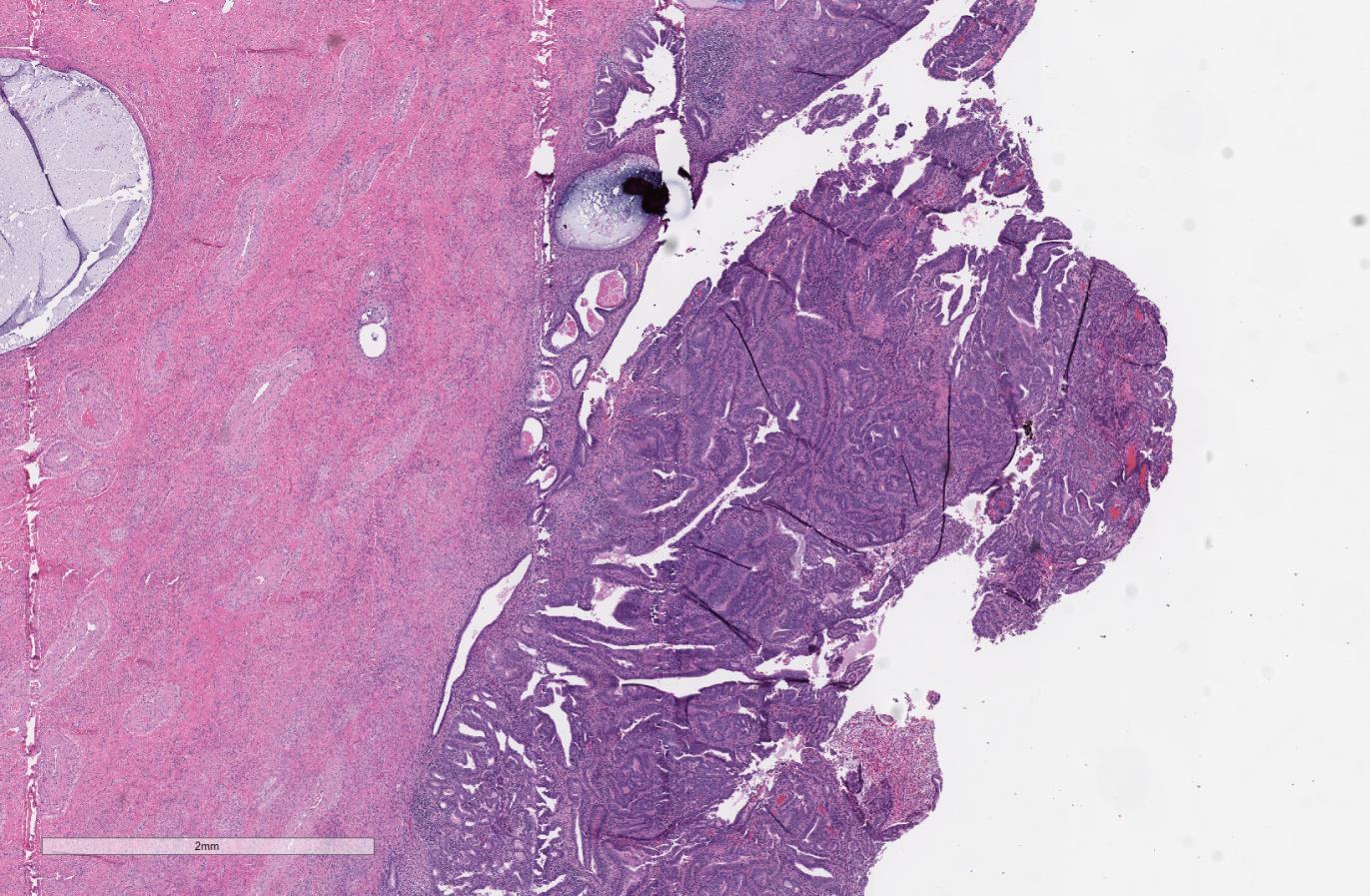
Figure 1 - Portion of posterior lower uterine segment with Endometrial Adenocarcinoma, Endometroid Type, FIGO grade 1.
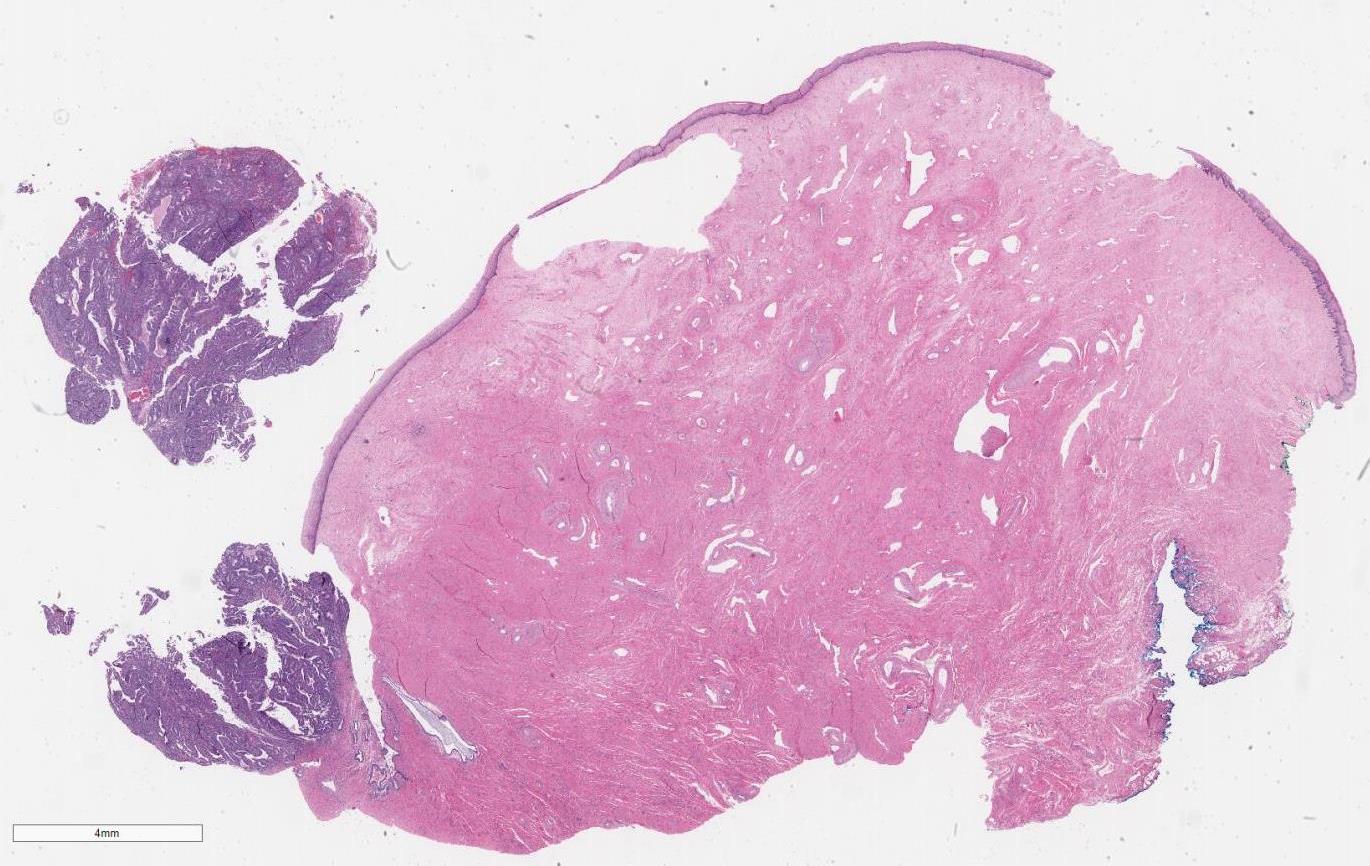
Figure 2 - Section of cervix with a polyp that appears very cellular with back to back gland formation (0.6x).

Figure 3 - Endocervical polyp involved by endometrial adenocarcinoma, endomertoid type, FIGO grade 1.
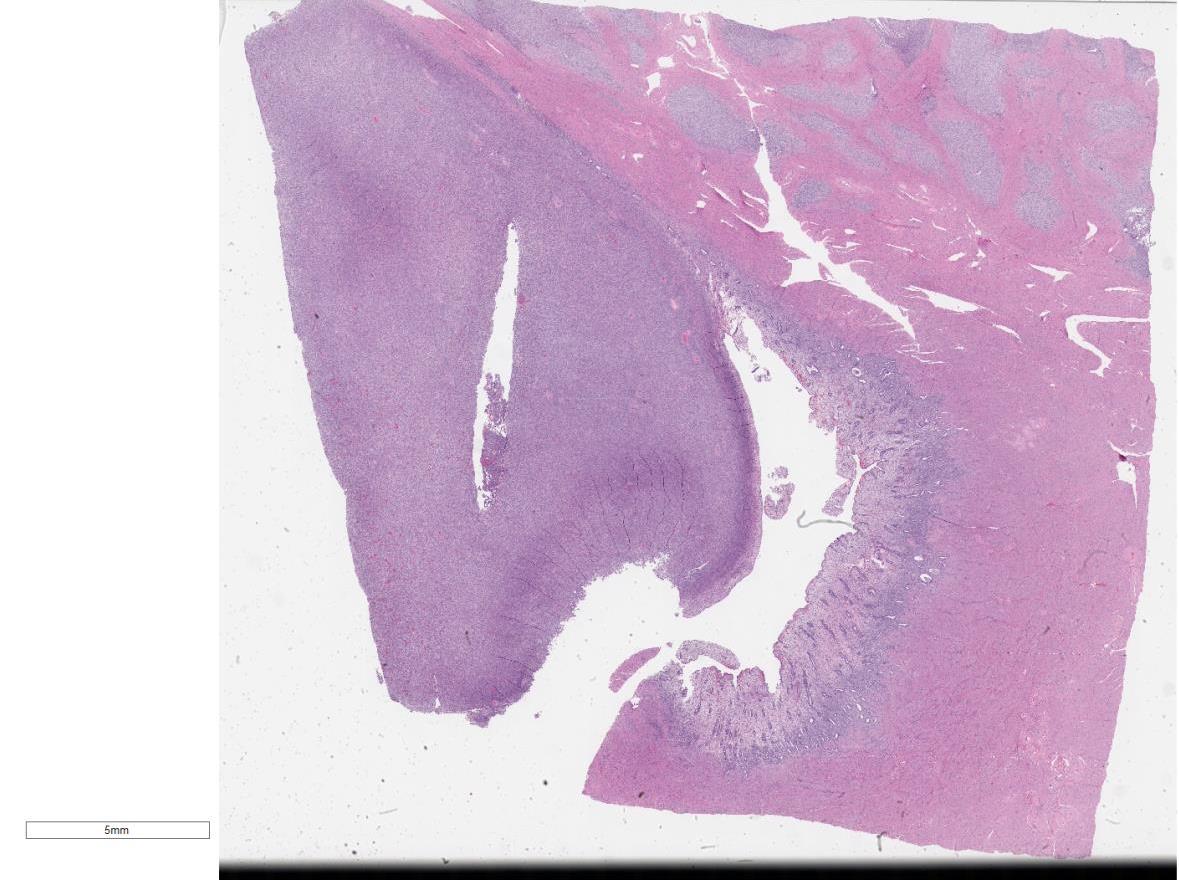
Figure 4 - Posterior uterine mass with a densely cellular exophytic portion and a portion with tongue-like cellular nests invading the myometrium (0.4x).

Figure 5 - Sheets of spindled cells in the exophytic portion of the posterior uterine mass (20x).
What is the diagnoses?
Choose one answer and submit.
C. Low grade endometrial stromal sarcoma and endometrial adenocarcinoma, endometroid type
> Learn more about this diagnosis.
 Meet our Residency Program Director
Meet our Residency Program Director