
Residency Program - Case of the Month
April 2018 - Presented by Raymond Gong (Mentored by: John Bishop)
Clinical History
The patient is a 69-year old woman who presented with a longstanding, recently enlarging left thyroid nodule. The patient initially elected for observation after having the nodule first evaluated in 2006. Serial ultrasounds over the years showed that the nodule had remained stable. However, the patient noted growth in the nodule over the last half-year and, in early 2018, was referred to Endocrine Surgery at the UC Davis Medical Center after developing vocal changes due to a dysfunctional left vocal fold. Other symptoms at this time included mild left neck pain and occasional dysphagia. The patient reported no family history of thyroid disorders and she denied any history of hyper- or hypothyroidism as well as any trauma, surgery, or radiation to the neck.
Ultrasound of the neck revealed a large heterogeneous mass with micro-calcifications in the lower pole of the left thyroid lobe within close proximity to the esophagus, trachea, and neck musculature. No cervical lymphadenopathy was noted. Fine needle aspiration of the thyroid nodule revealed extensive necrosis and cellular degeneration with scattered, pleomorphic cells. These cells were noted to have enlarged nuclei, occasional prominent macro-nucleoli, and irregular nuclear membranes.
After having reviewed her treatment options, the patient elected for total thyroidectomy with central neck dissection. Intra-operatively, the recurrent laryngeal nerve and cricothyroid muscle margins were negative. Final margins were negative and there was no evidence of metastasis to the lymph nodes.
Gross Description
The left thyroid lobe was largely replaced by a multilobulated, poorly-circumscribed, tan-white to yellow tumor with mixed firm, fleshy, and necrotic cut surfaces. The mass measured 5.6 x 3.7 x 2.7 cm and grossly appeared to abut the thyroid capsule.
Microscopic Description
Sections of the mass demonstrated both insular (Figure 1) and solid growth patterns with significant areas of necrosis (Figure 2). The tumor cells displayed vesicular, occasionally convoluted nuclei with mild nuclear pleomorphism and prominent nucleoli (Figure 3). Areas of solid growth showed a comparatively greater degree of pleomorphism and consisted of tumor cells showing spindle cell morphology (Figure 4). Immunohistochemical staining for CD56 and synaptophysin were negative in tumor cells. Thyroglobulin was positive in a minor subset of tumor cells (Figure 5).
Click on image to enlarge.

Figure 1: Low power view of the tumor's insular growth pattern, 100x
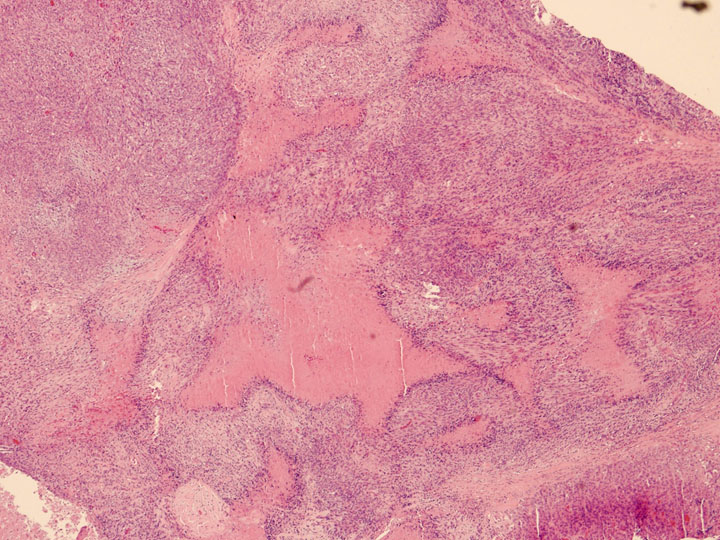
Figure 2: Low power view of the tumor's solid growth pattern with adjacent areas of necrosis, 40x
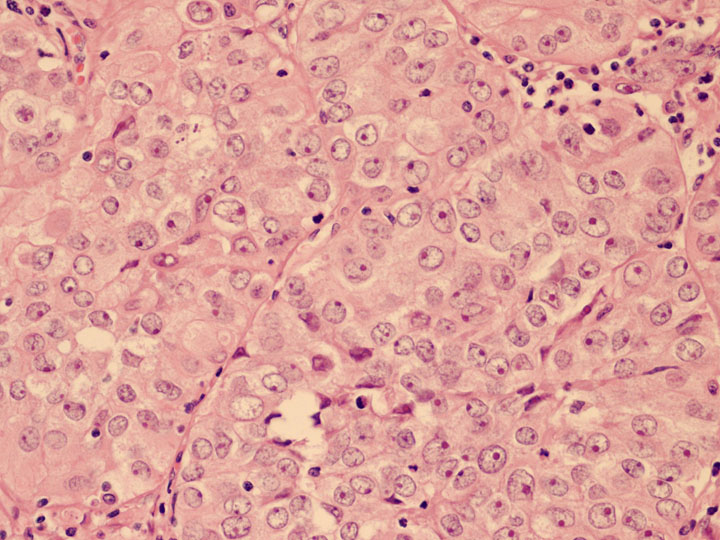
Figure 3: High power view of tumor cells, 400x
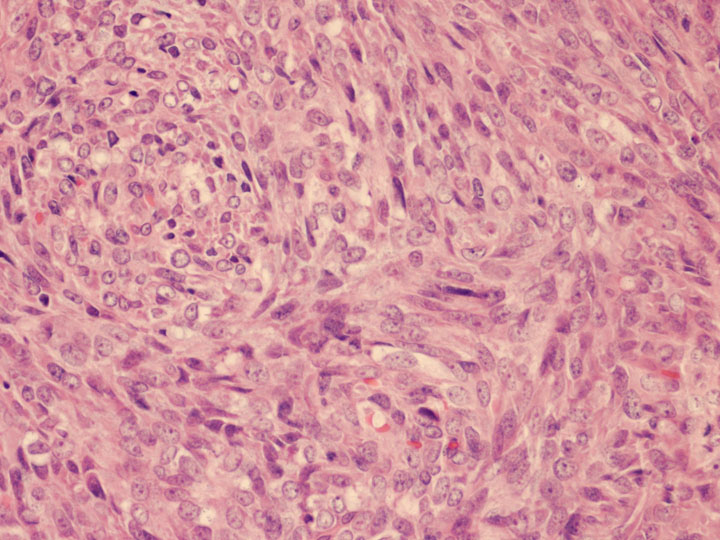
Figure 4: High power view of tumor cells with spindle cell morphology, 400x
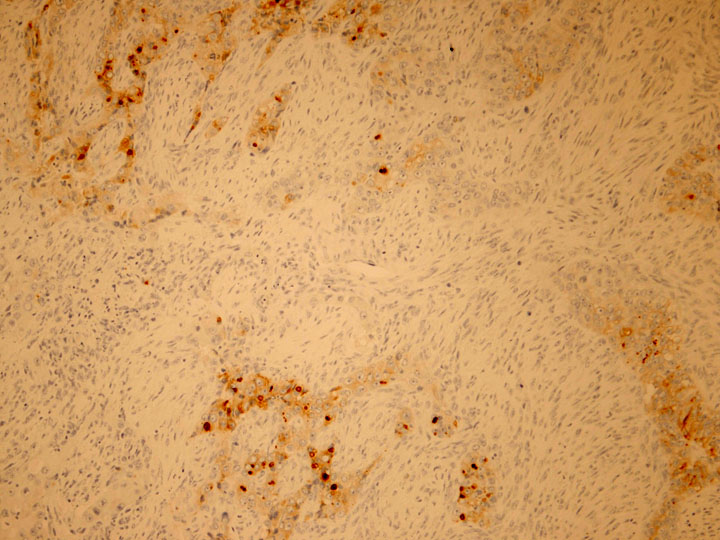
Figure 5: Thyroglobulin was positive in a minor subset of tumor cells, 100x
What is the diagnosis?
Choose one answer and submit.
 Meet our Residency Program Director
Meet our Residency Program Director