
June 2020 – Presented by Luke Dang (Mentored by Morgan Darrow)
Clinical History:
The patient is a 55-year-old man with chest pain and dyspnea after a ground-level fall. He also reports persistent generalized body pain over the past year. His past medical history includes hypertension, hyperlipidemia, diabetes, and coronary artery disease.
Imaging Findings:
A CT scan of the chest showed numerous bilateral rib fractures and a mass in the sternum (Figure 1). Additional imaging showed femoral, scapula, and pubic rami fractures. A PET scan showed areas of FDG avidity in the maxillary sinus as well as in the sternal mass (Figure 2).
Clinically, the constellation of findings is concerning for tumor-induced osteomalacia. Laboratory studies show elevated serum FGF-23 and low serum phosphorus, supporting this clinical impression. The maxillary sinus lesion was biopsied first and reported as an EBV-positive non-keratinizing undifferentiated nasopharyngeal carcinoma. As this tumor type is not known to be associated with tumor-induced osteomalacia, a biopsy of the sternal lesion was pursued.
Microscopic Description:
The lesion is composed of sheets of cytologically bland round to spindle-shaped cells involving bone (Figure 3). There is abundant vasculature throughout the lesion (primarily small capillaries). Focal calcifying matrix with a “grungy” appearance is observed (Figure 4). The lesional cells are positive for FGF23 mRNA via chromogenic in-situ hybridization (Figure 5).
Figure 1
Figure 2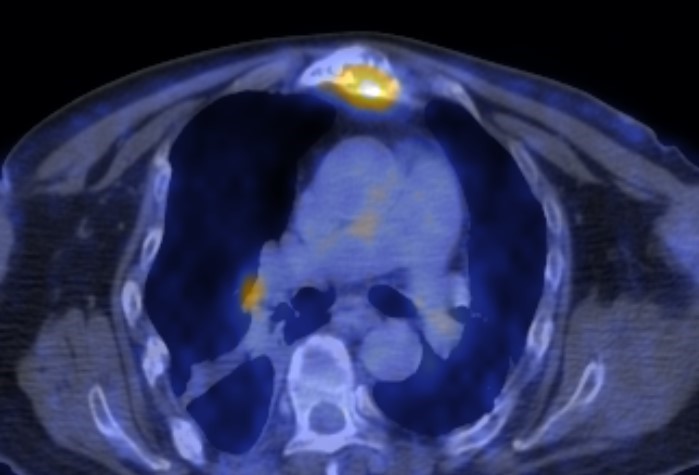
Figure 3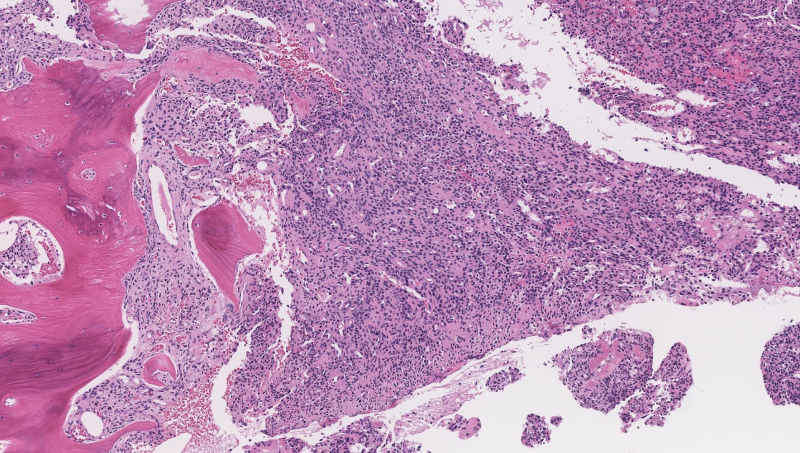
Figure 4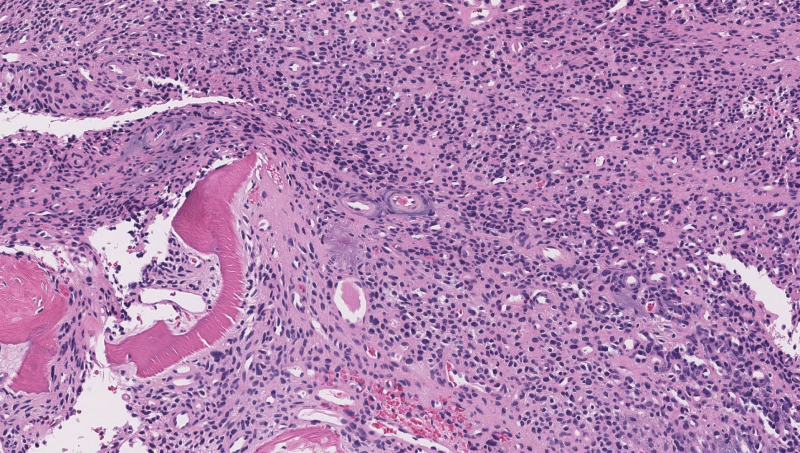
Figure 5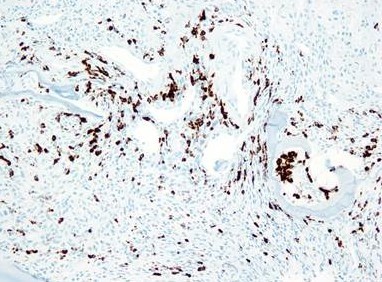
 Meet our Residency Program Director
Meet our Residency Program Director