
July 2022 – Presented by Dr. Alexander Ladenheim (Mentored by Dr. Tony Karnezis)
Clinical History and Gross Examination
A 70-year-old female with a history of postmenopausal hormone replacement therapy presented with postmenopausal bleeding, and endometrial biopsy showed endometrioid endometrial adenocarcinoma, FIGO grade 1. The patient underwent total laparoscopic hysterectomy and bilateral salpingoophorectomy.
On gross examination of the resection specimen, a 3.6 cm exophytic, friable mass of the uterine corpus was seen located 1.3 cm from the internal os with invasion to a depth of approximately 40% of the thickness of the myometrium. In addition, there was a 0.9 cm tan polyp of the endocervix. The cervix was otherwise grossly unremarkable.
Microscopic Examination
Sections of the uterine corpus mass show a conventional appearing endometrioid adenocarcinoma, FIGO grade 2 (Figure 1). IHC staining for the mismatch repair proteins MLH1 and PMS2 (Figure 2) shows loss of nuclear expression in the majority of the uterine corpus mass.
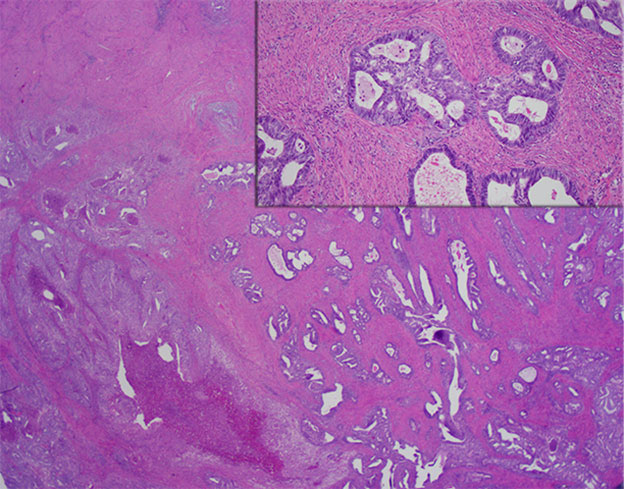
Figure 1: Endometrioid adenocarcinoma, FIGO grade 2, involving the uterine corpus (HE, 20x). Inset: Conventional cytologic features of endometrioid endometrial adenocarcinoma (HE, 100x)
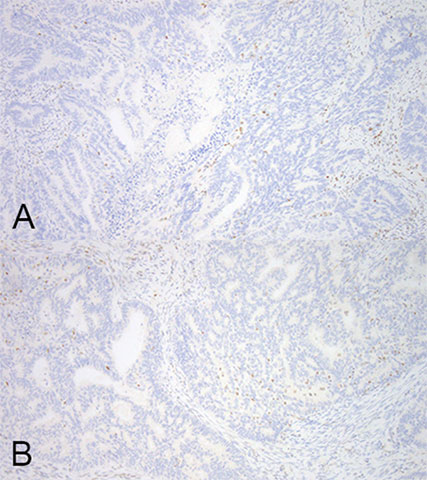
Figure 2: IHC staining of uterine corpus. A, MLH1 (100x) and B, PMS2 (100x)
Sections of the cervix showed the following:
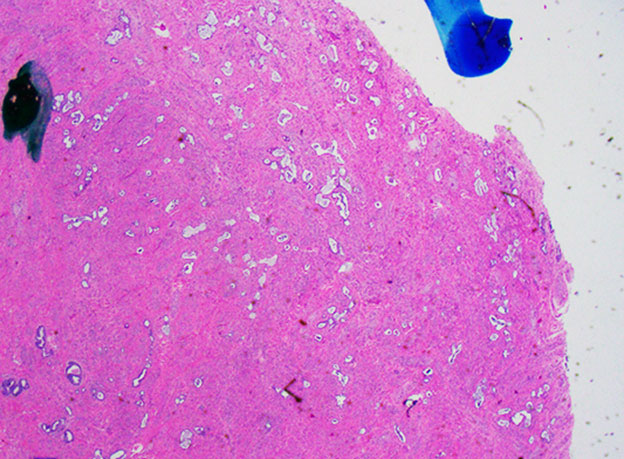
Figure 3: Cervix (HE, 20x)
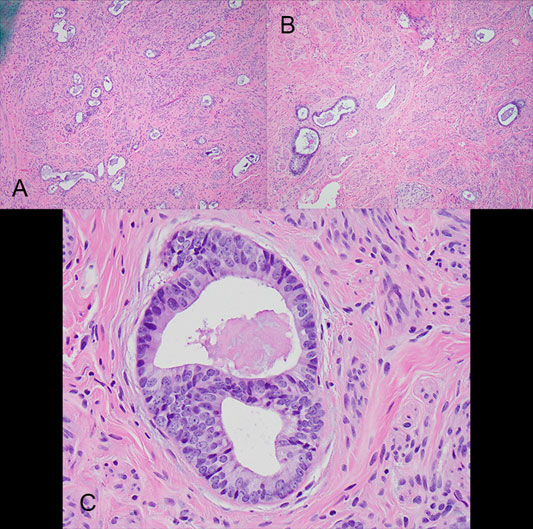
Figure 4: Cervix. A and B: HE, 100x, C: HE, 400x
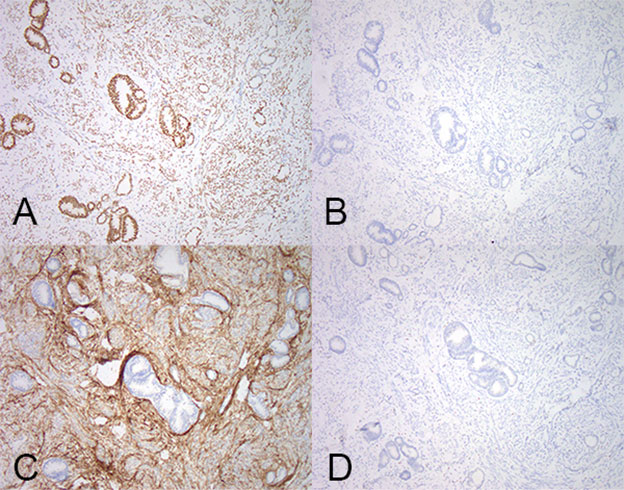
Figure 5: IHC staining performed on cervix. A: ER (100x), B: CEA (100x), C: CD10 (100x), and D: GATA3 (100x)
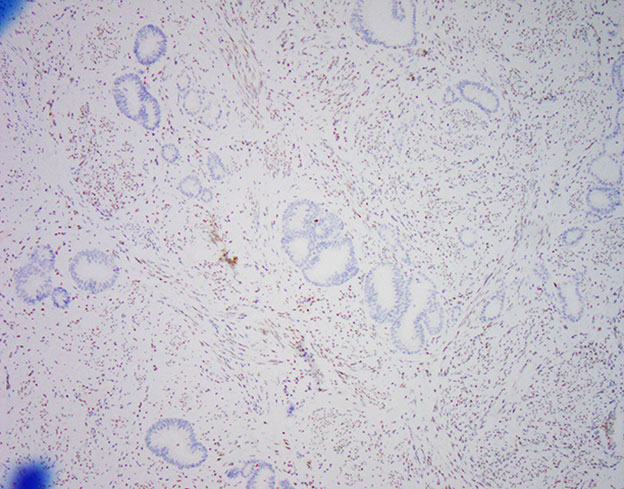
Figure 6: Cervix, MLH1 IHC (100x)
Additional IHC stains performed on the cervix and not shown: vimentin was positive throughout the epithelial component; p16 showed weak, heterogeneous staining; and p53 staining showed a wild-type staining pattern.
The correct answer is:
Sections of cervix revealed scattered, small, tubular glands with an infiltrative appearance (Figure 3) which are lined by cuboidal to columnar cells with luminal and intracytoplasmic mucin, pale nuclei with nuclear overlapping and pseudostratification, and distinct, often multiple, nucleoli (Figures 4A-4C). The glands are deeply infiltrative into the cervical wall. In some areas, the glands showed abnormal localization next to cervical stroma vessels (Figure 4B). These glands underlie normal appearing cervical surface epithelium and a benign endocervical polyp (not shown).
IHC staining of these glands was positive for ER (Figure 5A) and vimentin; and negative for CEA, CD10, and GATA3 (Figure 5B, 5C, and 5D). The glands had weak, heterogeneous expression of p16, and a wild-type p53 staining pattern. Staining for the mismatch repair proteins MLH1 (Figure 6) showed loss of expression in the majority of glands in the cervix, a similar pattern to that seen in the uterine corpus; methylation studies showed MLH1 promotor hypermethylation. Overall, the morphologic and immunophenotype is most consistent with stromal invasion of the cervix by endometrial adenocarcinoma (pT2).
 Meet our Residency Program Director
Meet our Residency Program Director