
August 2022 – Presented by Dr. Jacob Donnelly (Mentored by Dr. Meighan Tomic)
Clinical History
A 58-year-old male with a history of EtOH use disorder, gout, anemia, persistent atrial fibrillation, and HTN presented to the hospital for a fall and EtOH withdrawal. An incidental left lower quadrant mass was found on imaging. Subsequently, the tumor was excised with a small bowel resection.
Grossly

A large, firm, multinodular mass is present and has adhered two loops of small bowel. The mass has solid white to pale yellow cut surfaces and measures 6.8 x 6.4 x 5.7 cm. It grossly obliterates the muscularis propria and serosa of the two segments of bowel that are fused together. The mass does not grossly appear to involve the mucosa. It does extend into the mesenteric fat and is 2.3 cm from the mesenteric margin. Sectioning of the mesenteric fat reveals three white-tan, firm nodules that are separate from the primary mass, range in greatest dimension from 0.8 - 1.7 cm and are 1.6 cm in closest approach to the mesenteric margin.
Microscopy
Histologic sections of the small bowel masses demonstrate an abrupt transition between well differentiated and dedifferentiated components. The well differentiated component shows adipocytes with atypical nuclei. The dedifferentiated portion is cellular, showing pleomorphic spindle cells, with an increased mitotic rate.
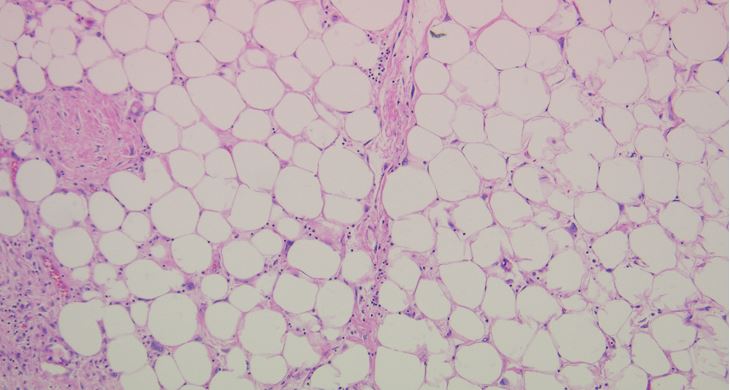
Figure 1. H&E 10X (Highlighting well-differentiated adipocytic component)
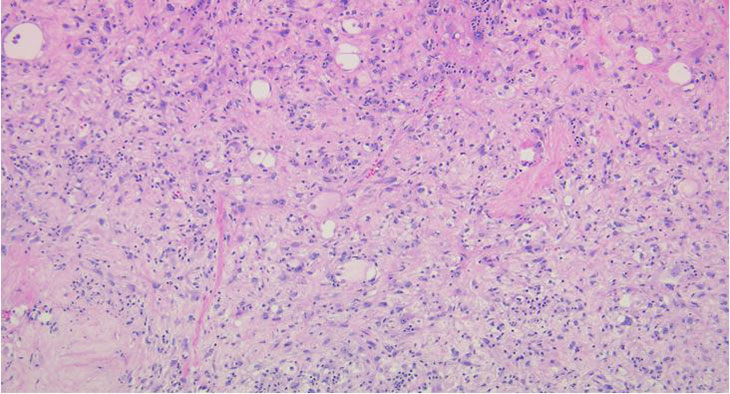
Figure 2. H&E 10x (Highlighting the high-grade component)
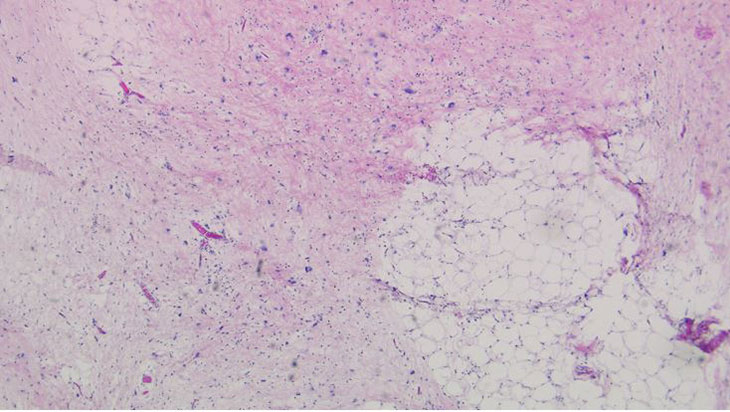
Figure 3. H&E 8x (Highlighting the transition from a well-differentiated adipocytic competent to a dedifferentiated area)
 Meet our Residency Program Director
Meet our Residency Program Director