
October 2022 – Presented by Dr. Anupam Mitra (Mentored by Dr. Morgan Darrow)
Clinical History
A 46-year-old female with past medical history of anemia presented to the emergency department complaining of a mass in her throat for last 3 months. Patient stated she was able to swallow food and liquids, but it has been difficult to manage secretions in the mouth. She has been seen in urgent care and prescribed a course of antibiotics without any improvement. She does not have any significant past medical history and denies fever, chills, shortness of breath or chest pain. She could not affirm any significant weight loss but seemed to have chronic malnutrition.
On examination, a left tonsillar mass was noted. On imaging a centrally necrotic mass is noted in the left palatine tonsil with conglomeration of cervical lymph nodes. Imaging of whole body showed a centrally necrotic solid mass in the lower lobe of left lung, another solid mass in the liver and two masses in the posterior body wall. These findings raised suspicion for a metastatic neoplasm. A biopsy of the tonsillar mass was performed. Multiple fragments of friable tan-red soft tissue were received and submitted entirely for microscopic examination.
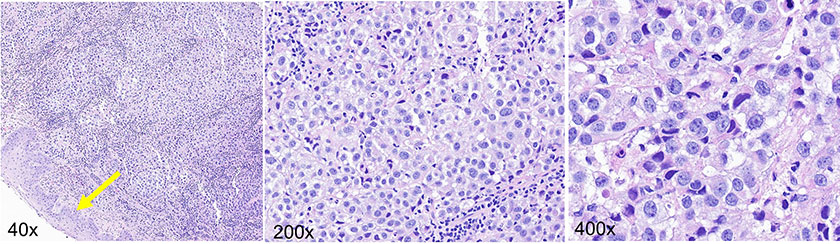
Histologic evaluation of the tissue revealed cytologically malignant cells arranged in sheets and clusters replacing the tonsillar lymphoid tissue without affecting the surface epithelium. The cells have mild to moderate pleomorphism with prominent nucleoli and amphophilic cytoplasm. Mitoses are readily identifiable. No pigment is present. The uninvolved surface epithelium is highlighted by a yellow arrow.
These histologic findings raise a differential diagnosis which includes non-keratinizing squamous cell carcinoma, lymphoma, and melanoma. A panel of immunohistochemical stains was performed and the findings are shown below.
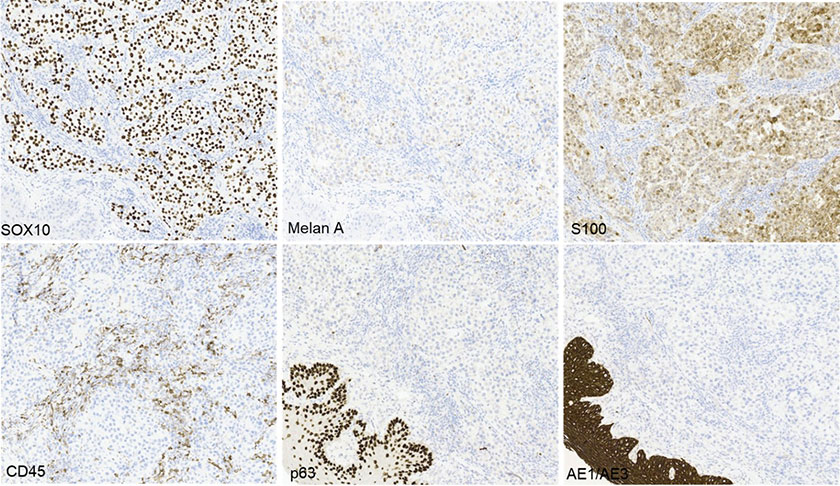
The tumor cells are positive for S100, SOX10 and Melan A (patchy) while negative for AE1/AE3, CK5/6, p63, p16, HMB45 and CD45. AE1/AE3, CK5/6 and p63 highlight the surface epithelium only. Based on the morphology and immunohistochemical staining pattern, the findings are consistent with melanoma involving the tonsillar tissue. The patient does not have any history of melanoma and no skin lesions were noted. Thus, this tonsillar lesion is most consistent with a primary mucosal melanoma.
Subsequently, the left lung nodule was biopsied and showed a similar histologic appearance and immunohistochemical stain profile as the tonsillar mass, compatible with metastatic melanoma. Palliative radiotherapy was initiated.
Mucosal melanoma (MM)
MM is a malignant neural crest-derived neoplasm with melanocytic differentiation. Usually, it is seen in older patients with a slight male predominance. It is a rare entity comprising <1% of all melanomas and <0.5% of all oral neoplasms. Metastasis to the oral cavity is even rarer than primary melanoma. MM most often involves the hard palate and maxillary alveolus followed by mandibular gingiva, buccal mucosa, and floor of mouth/tongue.
Lymph node involvement and distant metastasis are seen in almost half of the cases. Surgical excision, neoadjuvant therapy, and palliative radiation are the treatment choices. The overall prognosis of MM is poor with median survival of 2 years and 5-year survival of 5-10%.
 Meet our Residency Program Director
Meet our Residency Program Director