
Residency Program - Case of the Month
January 2018 - Presented by Ananya Datta Mitra (Mentored by Alaa Afify)
Clinical History
A 77-year-old G4P4004 female presented for evaluation of post menopausal bleeding. She had complaints of daily vaginal spotting for the past one month.
Her past medical history was notable for H/O right breast invasive ductal carcinoma (stage II, T1b N1). In June 2003, she underwent right lumpectomy and sentinel lymph node biopsy, revealing a 1 cm, intermediate grade infiltrating ductal carcinoma. One of 2 sentinel lymph nodes was positive. However, the patient declined further axillary lymph node dissection. Her tumor was hormone receptor positive with less than 5% estrogen receptor staining, and 80% progesterone receptor staining. She declined adjuvant chemotherapy. She was started on radiation therapy which she completed in October of 2003. She received nearly 8 years of adjuvant endocrine therapy, including tamoxifen from August 2003 until October of 2005. She was then switched to the aromatase inhibitors and completed endocrine therapy in April 2011. She tested negative for BRCA1 and 2 mutations in 2003.
She has had previous endometrial biopsy in June of 2013 for postmenopausal bleeding, which showed scant fragments of inactive surface endometrium with no evidence of endometrial intraepithelial neoplasia (EIN) or malignancy. Since early November of 2016, she started having increased vaginal bleeding which prompted her to seek medical attention. Endometrial biopsy on January 2017 showed endometrial adenocarcinoma, endometrioid type, consistent with FIGO grade 1. It was also noted that in addition to the endometrioid adenocarcinoma (PAX-8 positive) there are malignant cells seen that are GATA3 immunohistochemistry positive which are suspicious for metastatic breast cancer. To complicate her case further she was also diagnosed with a biopsy proven melanoma in situ in the left shin in October 2016.
The patient then underwent total laparoscopic hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic lymphadenectomy on February 2017.
Gross Findings
The resected specimen weighed 112g and consisted of uterus, bilateral ovaries and fallopian tubes. The endometrial cavity (3.8 cm from cornu to cornu x 5.2 cm in length) has an exophytic, friable, tan polypoid mass measuring 2.9 x 2.7 x 1.6 cm, that involves the anterior endometrium near the fundus, and is 2.5 cm from the internal os (Figure 1). The uninvolved endometrium is tan/pink and smooth (0.2 cm in average thickness). The tan coarsely trabeculated myometrium measures 1.4 cm in maximum thickness.
Click on image to enlarge.
Figure 1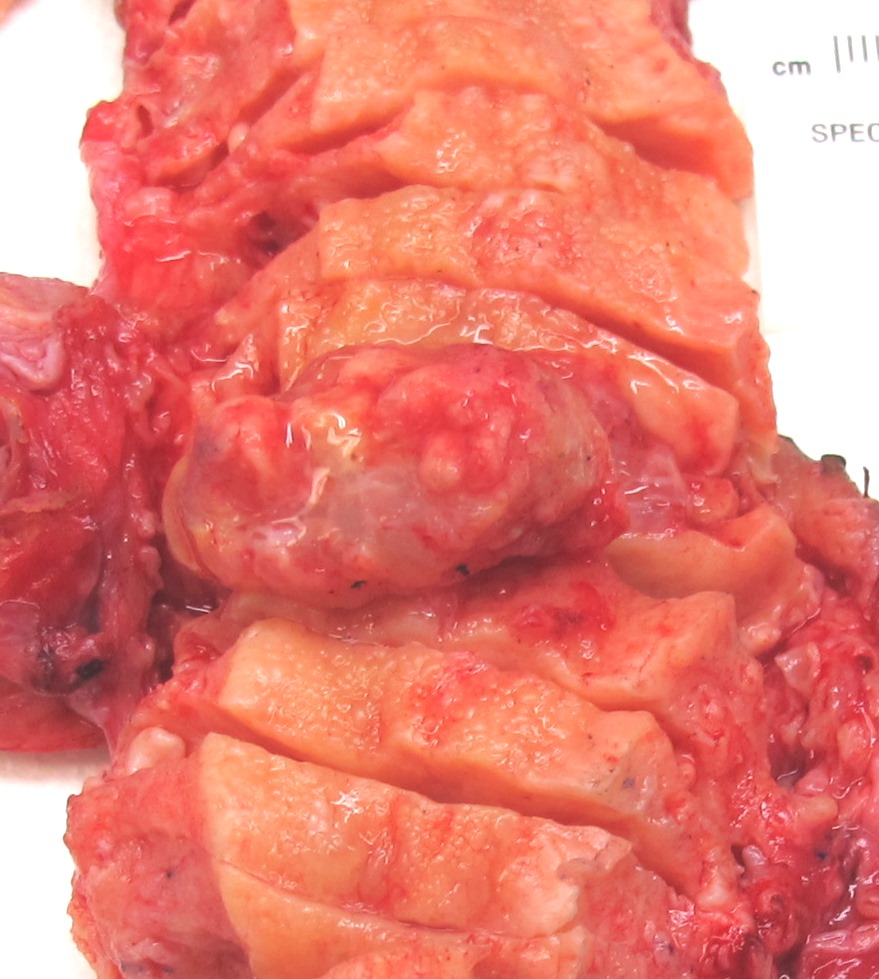
Microscopic Findings
Microscopically the tumor is biphasic with malignant glandular component as well as malignant stromal component (Figure 2).
Click on image to enlarge.
Figure 2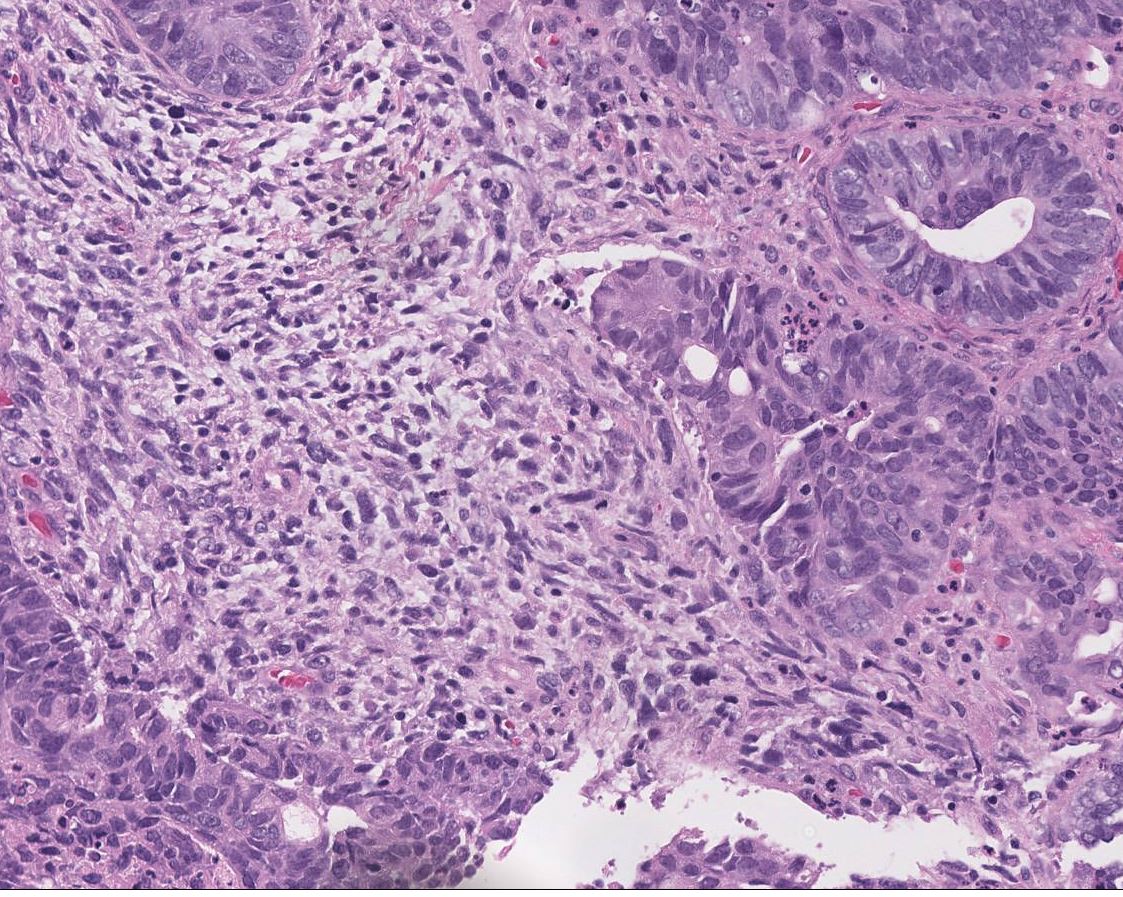
Immunohistochemical Staining
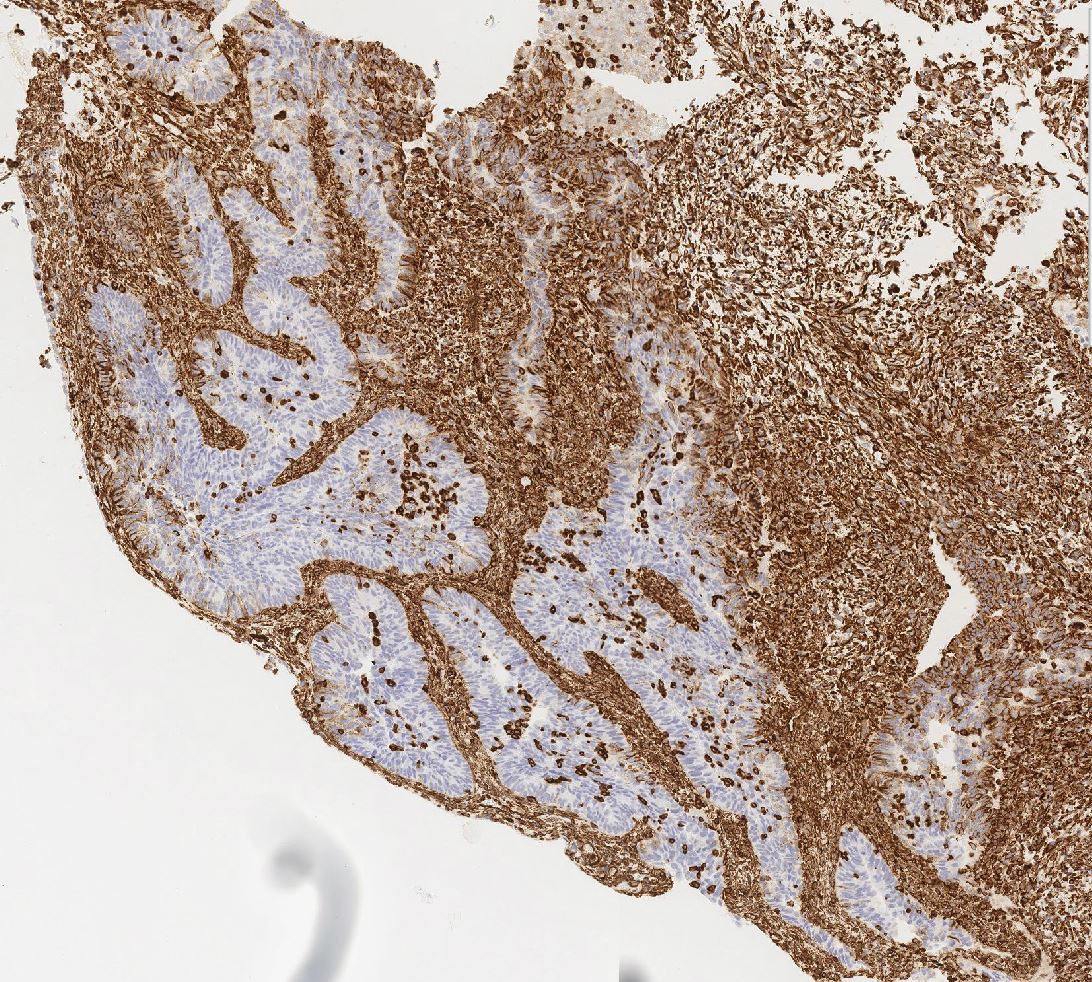
Immunohistochemical stains performed and interpreted at U.C. Davis Medical Center revealed the following results in the area of interest (Figure 4-5).
Click on image to enlarge
| Figure 3 | Figure 4 | Figure 5 | ||
 |
 |
 |
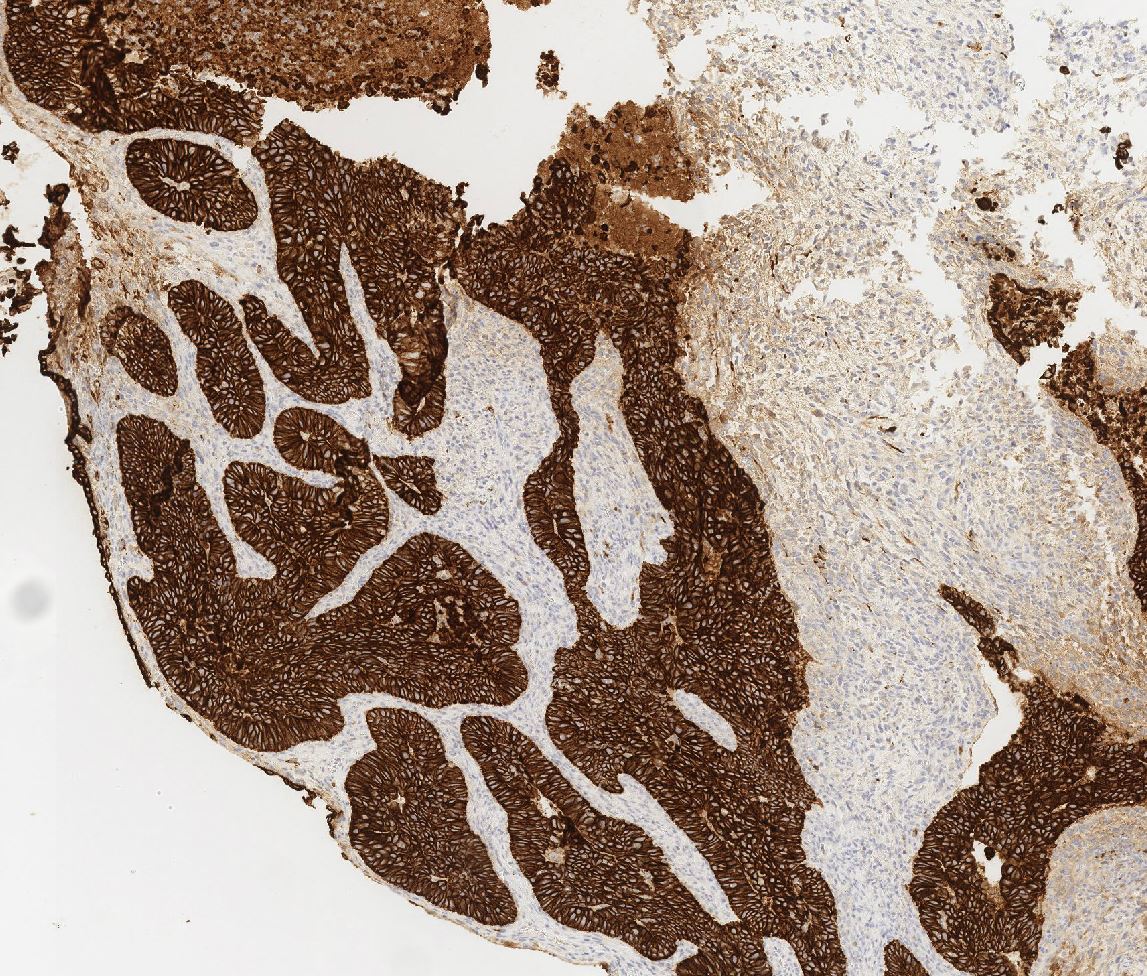
| AE1/AE3: | Figure 3, highlights epithelial component | |
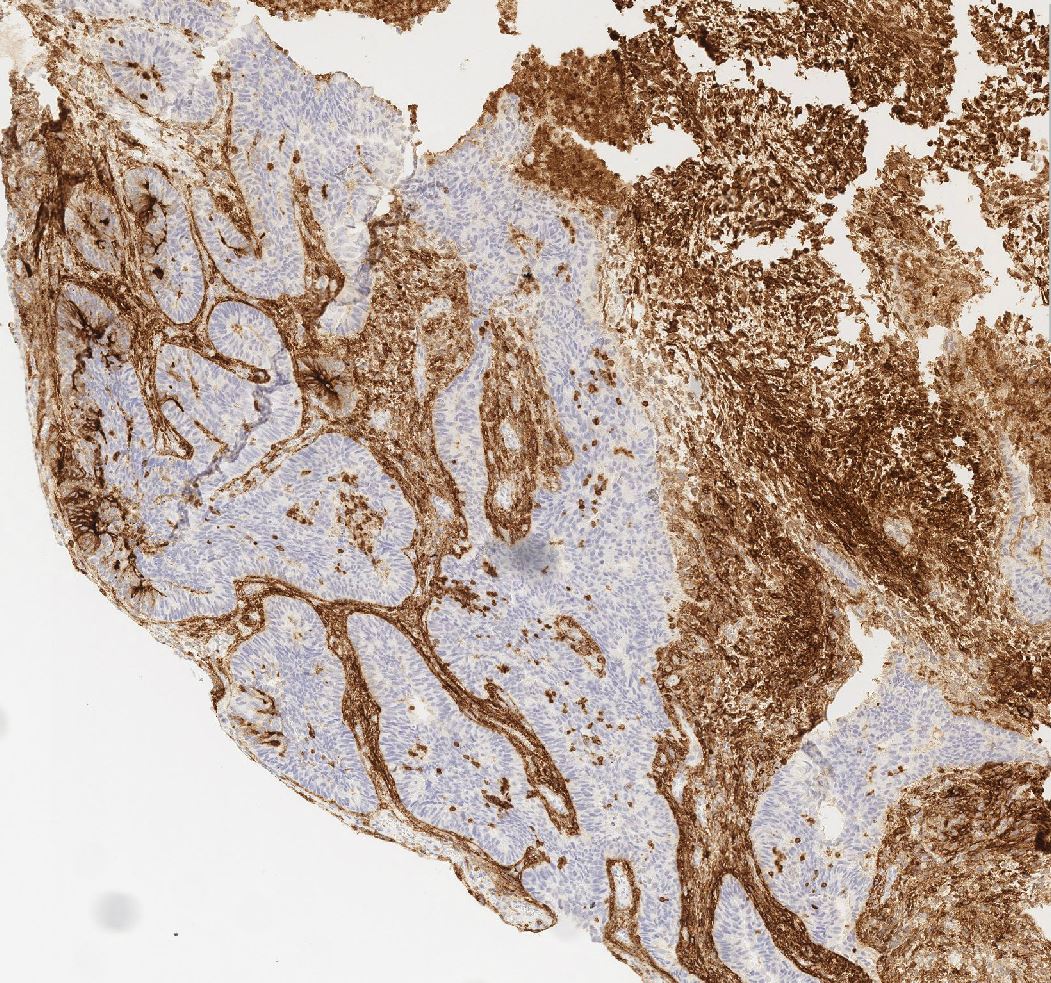
| CD10: | Figure 4, highlights sarcomatoid component | |
| Vimentin: | Figure 5, highlights sarcomatoid component |
What is most likely the diagnosis?
Choose one answer and submit.
A.) Carcinosarcoma (Malignant Mixed Mullerian Tumor, MMMT)
> Learn more about this diagnosis.
 Meet our Residency Program Director
Meet our Residency Program Director