
July 2020 – Presented by Raymond Gong (Mentored by Elham Vali Betts)
Clinical History:
A 70-year-old female with a past medical history of primary biliary cholangitis who developed liver failure at the age of 43 and underwent liver transplantation two years later at the age of 45 presented with progressive abdominal distension, early satiety, weight loss, and fatigue. Radiologic imaging was notable for multiple mesenteric and omental masses measuring up to 6 cm in greatest dimension. A representative omental mass was targeted for core needle biopsy under ultrasound-guidance.
Microscopic Description:
The core needle biopsy showed a diffuse proliferation of atypical lymphoid infiltrate with effacement of normal lymph node architecture composed of large cells (Figure 1). These cells demonstrated scant cytoplasm and large pleomorphic nuclei with one to multiple prominent nucleoli. Mitotic figures and apoptotic bodies were readily identified (Figures 2). Areas of necrosis were also noted (Figure 3).
Ancillary Testing:
A panel of immunohistochemical (IHC) stains was performed on the core needle biopsy to further characterize the neoplasm. Staining in the large neoplastic cells was interpreted as follows:
| IHC Stain: | Interpretation: | |
| AE1/AE3 | Negative | |
| CD3 | Negative | |
| CD5 | Negative | |
| CD20 | Positive | (Figure 4) |
| PAX5 | Positive | (Figure 4) |
| CD30 | Negative | |
| BCL-1 (Cyclin D1) | Negative | |
| BLC-2 | Positive | (Figure 5) |
| C-MYC | Positive | (Figure 5) |
| CD10 | Negative | (Figure 5) |
| BCL-6 | Positive, greater than 30% | (Figure 5) |
| MUM1 | Positive, approximately 30-40% | (Figure 5) |
| Ki-67 | High proliferation index, approximately 90% | (Figure 5) |
The patient’s Epstein-Barr virus (EBV) antibody profile was positive for IgG antibody against EBV nuclear antigen, viral capsid antigen, and early antigen and negative for IgM antibody against EBV viral capsid antigen. Her EBV viral load was less than 750 DNA copies per milliliter (reportable range: 750-7,500,000 copies/ml).
Testing of the core needle biopsy for EBV-encoded RNA by in situ hybridization (EBER-ISH) was negative.
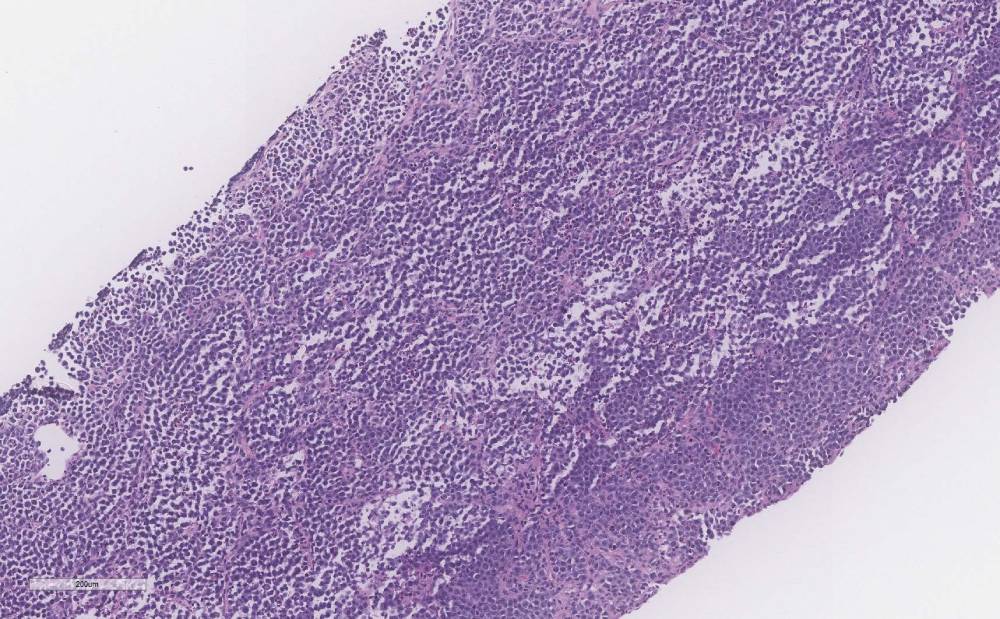
Figure 1: Low magnification view of a diffuse proliferation of large atypical cells with effacement of normal lymph node architecture (100x)
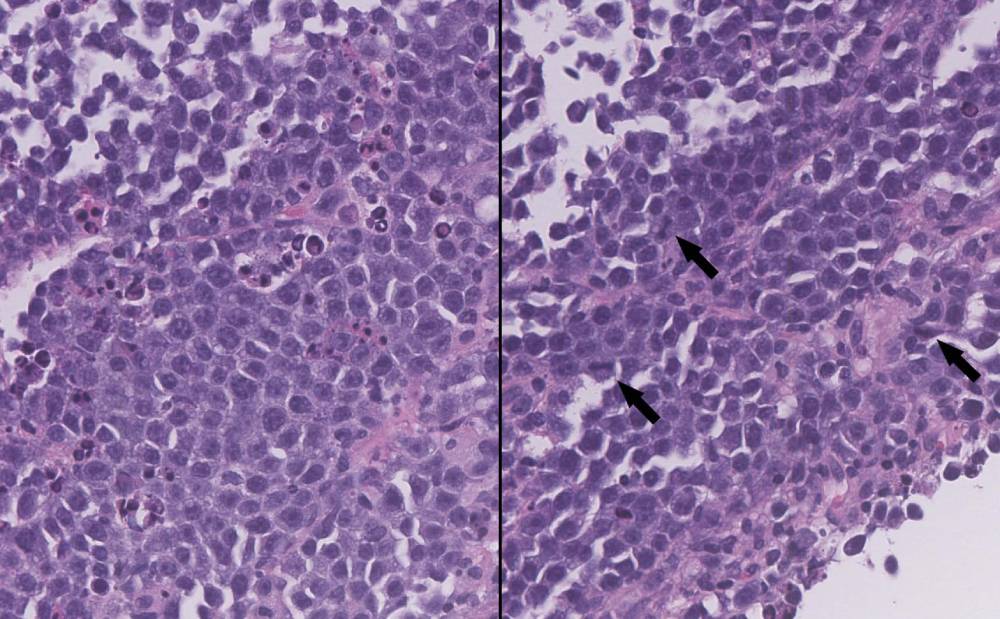
Figure 2: The large atypical cells exhibit a high nuclear-cytoplasmic ratio and large pleomorphic nuclei with prominent nucleoli. Cellular degeneration, apoptotic bodies, and mitotic figures (right, arrows) are readily identifiable (400x)
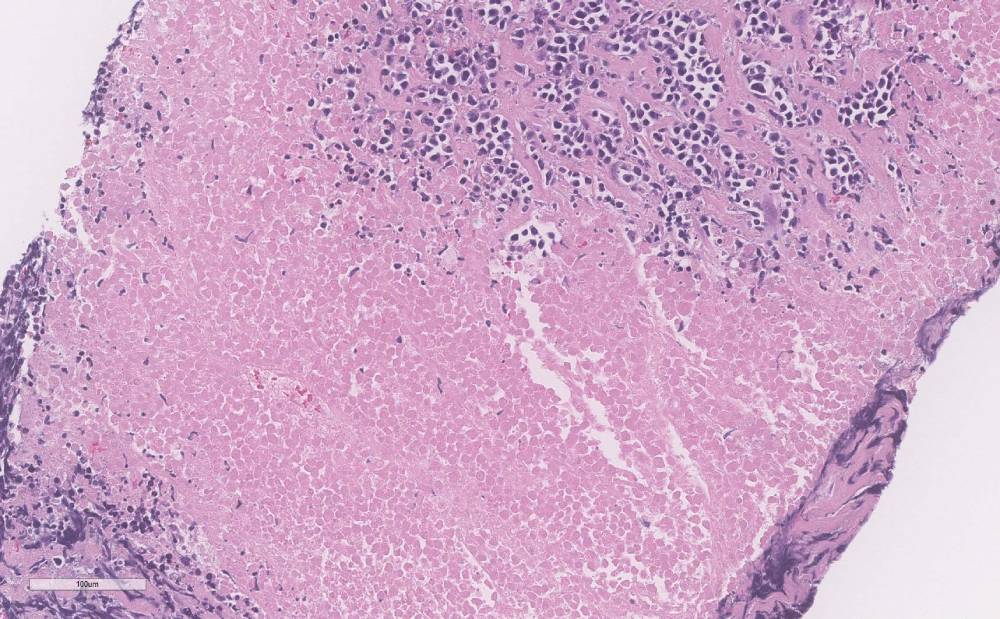
Figure 3: Prominent areas of necrosis are present (100x)
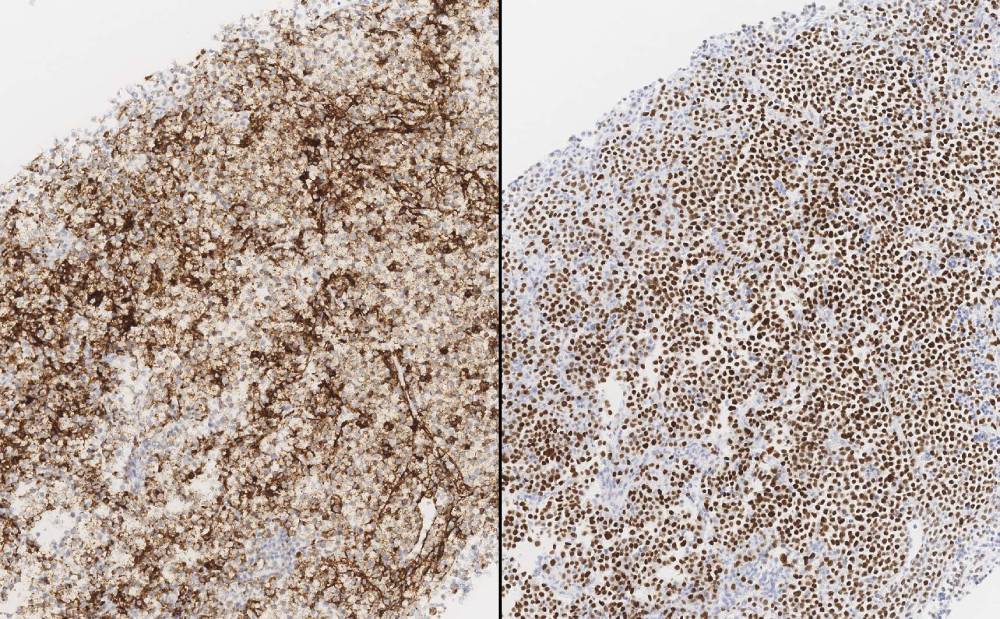
Figure 4: B-cell lineage markers CD20 (left) and PAX5 (right) are positive in the large atypical cells (100x)
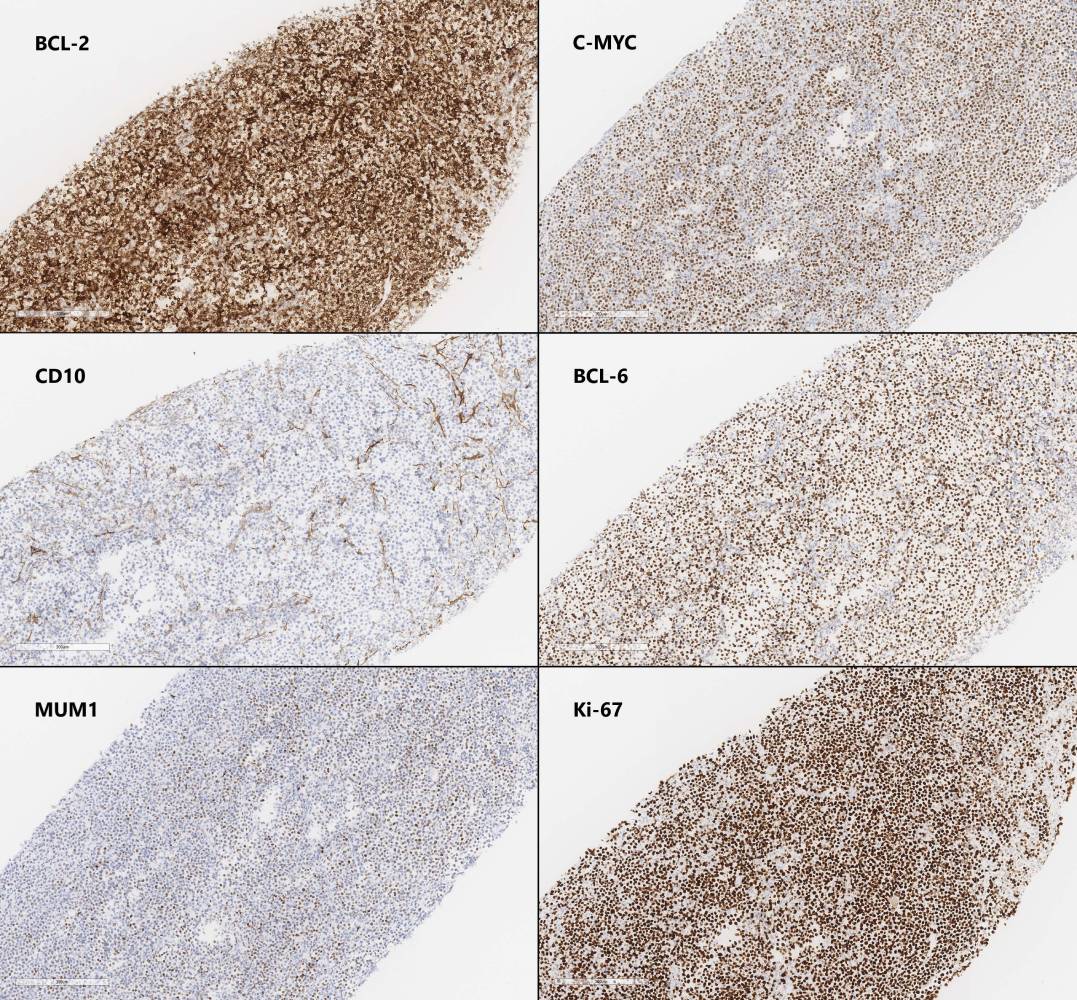
Figure 5: With the exception of CD10, IHC stains for BCL-2, C-MYC, BCL-6, and MUM1 are positive in the large atypical cells to varying degrees. Ki-67 staining demonstrates a high proliferative index. Refer to the “Ancillary Testing” section for an interpretation of the full IHC workup performed on this case (100x)
 Meet our Residency Program Director
Meet our Residency Program Director