A valuable home dialysis procedure for children with chronic kidney disease
By Tricia Tomiyoshi
(SACRAMENTO)
In an educational review published in the journal Pediatric Nephrology, clinicians at UC Davis and Oregon Health & Science University discuss an important procedure for children with advanced kidney disease: tidal continuous cycling peritoneal dialysis (TPD). The paper outlines the advantages of this approach and highlights several clinical nuances to help nephrologists embrace the procedure.
“Around 10% of children with chronic disease get TPD, but there’s a lot of confusion about the procedure and how to prescribe it,” said Lavjay Butani, chief of pediatric nephrology at UC Davis Health and first author of the paper. “We wanted to clarify some of the confusing guidelines and really go into the benefits.”
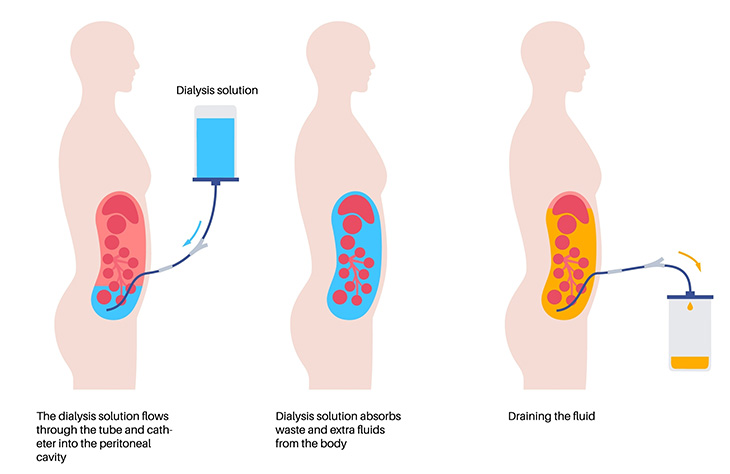
Illustration of the peritoneal dialysis procedure
Unlike hemodialysis, which pumps blood out of the body to be externally filtered, peritoneal dialysis uses the abdominal lining to naturally clear impurities from the blood. And while hemodialysis must be performed at a clinical facility, peritoneal dialysis can be performed at home.
The procedure uses a device called a cycler, which provides dialysis each night. The cycler is attached to a catheter in the child’s abdomen to remove impurities and excess fluid. In the paper, the authors draw distinctions between the two forms of peritoneal dialysis: continuous cycling (CCPD) and TPD.
“Instead of completely emptying the abdomen of the dialysis fluid, which is what you typically do with CCPD, TPD leaves a little bit inside to bathe or float the catheter,” said Butani. “The main advantage is that it reduces discomfort, which can be a substantial barrier to successful dialysis.”
During the night, the dialysis is performed multiple times. By leaving a little fluid in the abdomen, and only draining completely every three or four cycles, TPD helps keep the catheter in place. This can dramatically reduce pain. By making this nightly procedure more comfortable, TPD can potentially increase compliance and improve patients’ health.
While the literature review confirmed that TPD reduces pain compared to CCPD, there was little evidence to show that it more effectively removes waste. However, it may benefit kids undergoing high-volume dialysis or those who have a lot of fluid in their abdomens.
The authors note that there are no obvious disadvantages to TPD, as long as it is done properly. For example, the fluid must be completely drained every few cycles, or it can build up and cause discomfort. The paper also provides numerous insights to help nephrologists write the most effective TPD prescriptions.
“We feel this type of home dialysis is effective and improves quality of life for pediatric patients,” Butani said. “We hope nephrologists will become more familiar with TPD and prescribe it more frequently, as appropriate, for their patients.”
The co-authors of this paper are Maha Haddad of UC Davis Health and Mark Joseph of Oregon Health & Science University.